


Sevcan Fata1*, Merlinda Aluş Tokat2, Neşe Bağardı3, Bülent Yılmaz4
1 Research Assistant Doctor, Nursing Faculty, Dokuz Eylul University, Izmir, Turkey, ORCID ID: 0000-0002-0023-5884
2 Associate Proffesor, Nursing Faculty, Dokuz Eylul University, Izmir, Turkey, ORCID ID: 0000-0002-5899-0524
3 Nurse, Tepecik Training and Research Hospital, Izmir, Turkey, ORCID ID: 0000-0002-3576-4452
4 Doctor, Katip Celebi University Hospital, Izmir, Turkey, ORCID ID: 0000-0002-9458-2253
*Corresponding Author: Sevcan Fata, Research Assistant Doctor Sevcan Fata, Gynecology&Obstetrics Nursing Department, Nursing Faculty, Dokuz Eylul University, Izmir, Turkey
Abstract
Background: Infertility the treatment process for women becomes more stressful with tests for diagnosis and treatments.
Objectives: This study aimed to ascertain the reasons for the infertility-related stress and most stressful time in the infertility diagnosis and treatment process.
Materials & Methods: In this retrospective cohort study, data were collected from 154 infertile women in Izmir In Vitro Fertilization Clinic by using “Socio-Demographic and Infertility Characteristics Questionnaire” and “Reasons of Infertility-Related Stress and Most Stressful Time Questionnaire”.
Results: The 31.2% of participants had a female factor, 27.9% had unexplained infertility. In diagnosis progress, 88.3% of the women experienced stress. The most common reason for infertility-related stress was questioned about the diagnosis from neighbors (75.0%). It was determined that the most stressful time for women in the diagnosis process was when they expected test results related to the diagnosis (40.5%). During the treatment process, 89.0% (n: 137) of women stated that they experienced infertility-related stress. Questions from neighbors related to treatment (62.8%) were included as the most frequent conditions that cause stress during the treatment process.
Conclusion: Determining the stress reasons and the most stressful time and providing appropriate support for women may reduce the stress they in the diagnosis and treatment process.
Keywords: Infertility-related stress, reasons of infertility-related stress, most stressful time.
Introduction
Stress is a person's reaction to protect himself from external threats. It negatively affects women physiologically and psychologically, thereby reducing the likelihood of fertility [1]. Studies have reported that infertile women have significant stress [2,3]. This stress makes it difficult for fertility treatment, decreases its effectiveness, and negatively affects the outcome of treatment [4-8]. Also, as stress can negatively affect the treatment process, the treatment process also increases stress. The infertility process for women becomes stressful with tests for diagnosis and treatments. Most of the evaluations made at the stage of diagnosis include only women. In the treatment phase, since the woman will continue the pregnancy, many applications are made to the woman to prepare her body for pregnancy [9]. In a study with women who experienced assisted reproductive techniques (ART), it has been determined that the processes involving waiting for the test results related to infertility, starting fertility treatment, oocyte pick-up (OPU), waiting for the result after embryo transfer, and learning the negative test result were quite stressful [5]. Other studies have shown that infertile women experience stress during the diagnosis and treatment of infertility, the causes of stress are due to economic, social pressure, and productivity loss, and they experience stress mostly during treatment procedures and waiting for results [10-12]. There are studies in the literature of the world and our country regarding stress experience, stress level, factors affecting stress, and ways to cope with stress. In this study, unlike the literature, it is aimed to identify the reasons for infertility-related stress and the most stressful time in the diagnosis and treatment phase, separately, to manage stress and to make individual attempts. Thus, more effective interventions can be planned by determining when and why infertile women experience stress throughout the process.
Material & Methods
Design and population
It was a retrospective cohort study. Women undergone at least one ART cycle at Training and Research Hospital IVF Clinic in Izmir, between May August 2016 were recruited to this study. In this clinic, infertile women are examined, diagnostic tests and treatments are applied. The average number of monthly patients that visit the clinic is 50. The GPower 3.0.1 statistics program was used to determine the sample size. This analysis was based on the descriptive study conducted by Karaca & Ünsal with 118 infertile women, the stress level, and the influencing factors were examined [2]. As a result of the analysis, the number of samples was calculated as 32. It is planned to participate in at least 100 infertile women to increase the sample power. The women who met inclusion criteria participated in this study. The inclusion criteria were women (1) diagnosed with primary or secondary infertility, and (2) completed at least one ART cycle. (1) continuing diagnosis or treatment process, (2) women with literacy or language problems, and (3) pregnancy were exclusion criteria for participation.
Instruments
All women who fulfilled the inclusion and exclusion criteria were counseled regarding study enrolment by oral and written information and signed written informed consent. They then received “Socio-Demographic and Infertility Characteristics” and “Reasons of Infertility-Related Stress and Most Stressful Time Questionnaire”.
Socio-Demographic and Infertility Characteristics Questionnaire: It includes sociodemographic questions such as age, marriage, education level, working, and being able to take time off from work; infertility-related questions such as the cause and type of infertility, duration of infertility and duration treatment process.
Reasons of Infertility-Related Stress and Most Stressful Time Questionnaire: It was created in accordance with the literature regarding infertility-related stress during the diagnosis and treatment process. A total of three main questions were included in this questionnaire; whether women experience infertility-related stress, the reasons for infertility-related stress, and the most stressful time. These three main questions were asked separately for the diagnostic process and for the treatment process. The reason we asked few questions as to not raise their anxiety by using too many long surveys that could remind these women of negative processes. Before the questionnaire was applied to women, it was presented to 2 infertility specialists, 3 infertility nurses in the IVF center where the study was conducted, and 3 academicians who have publications in the field of infertility for expert opinion. The questionnaire, which was found appropriate as a result of expert opinion, was applied to 10 women and evaluated in terms of clarity.
Data collection
The data were collected by face-to-face interview techniques. Instruments were given to women who were diagnosed with infertility, completed at least one treatment cycle, were not pregnant, and came to the clinic to learn the test result or to make an appointment. Written consent, “Socio-Demographic and Infertility Characteristics Questionnaire” and “Reasons of Infertility-Related Stress and Most Stressful Time Questionnaire” were filled in respectively. The questions about diagnosis in “Reasons of Infertility-Related Stress and Most Stressful Time Questionnaire” were completed first, and then questions about treatment were continued. Data on both diagnosis and treatment process were obtained retrospectively.
Statistical analysis
Frequencies and percentages regarding whether women experience infertility-related stress, the reasons for infertility-related stress and the most stressful time in the diagnosis and treatment process were expressed in mean ± standard deviation (SD).
Ethical considerations
This study was approved by the university ethical board (Decision No: 2016/11‑16) and the hospital administration. As confidence is important in obtaining data related to fertility problems and stress, the researcher first verbally explained the aim of the research to participants and subsequently obtained their written consent.
Results
Sociodemographic characteristics and infertility history
The average age of women was 32.77, the average year of marriage was 7.91. The 33.1 % of women were high school graduates, the 57.8% not employed and, 55.2 % of employed women had difficulty in obtaining permission from employers related to diagnosis or treatment process. In fact, 5.2 % of women had to leave their jobs because they had difficulty in getting permission during the diagnosis and treatment process. When we look at the infertility factors, we recognized that 31.2 % of participants had a female factor, % 27.9 % had unexplained infertility (most associated with infertility-related stress in the literatüre). It was also determined that 46.8 % have been diagnosed 1-2 years ago, 33.8 % of them have been treated for 3-5 years and 81.8 % of them were primary infertile (Table 1).
Table 1: Socio-demographic and infertility characteristics (n: 154)
|
|
AVERAGE (MIN-MAX) |
STANDARD DEVIATION |
|
Age (years) |
32.77 (20.00-45.00) |
5.06 |
|
Marriage (years) |
7.91 (1.00-28.00) |
4.58 |
|
|
n |
% |
|
Education level Primary School |
38 |
24.7 |
|
Secondary School |
31 |
20.1 |
|
High School |
51 |
33.1 |
|
Undergraduate |
34 |
22.1 |
|
Employment |
|
|
|
Employed |
57 |
37.0 |
|
Unemployed |
89 |
57.8 |
|
Quitting due to treatment |
8 |
5.2 |
|
Getting permission from work* |
|
|
|
Forced |
32 |
55.2 |
|
Not forced |
26 |
44.8 |
|
Infertility factor |
|
|
|
Female |
48 |
31.2 |
|
Male |
43 |
27.9 |
|
Both female and male |
20 |
13.0 |
|
Unexplained |
43 |
27.9 |
|
Type of infertility |
|
|
|
Primer infertility |
126 |
81.8 |
|
Secondary infertility |
28 |
18.2 |
|
Duration of diagnosis |
|
|
|
1-2 years |
72 |
46.8 |
|
3-5 years |
54 |
35.1 |
|
6-10 years |
27 |
17.5 |
|
10 years or more |
6 |
3.9 |
|
Duration of treatment |
|
|
|
Less than 1 year |
22 |
14.3 |
|
1-2 years |
45 |
29.2 |
|
3-5 years |
52 |
33.8 |
|
6-10 years |
24 |
15.6 |
|
10 years or more |
6 |
3.9 |
* Employed women responded.
Reasons of the infertility-related stress and most stressful time during diagnosis and treatment process
Reasons of the infertility-related stress and most stressful time during the diagnosis process
The 88.3% (n: 136) of women stated that they experienced stress during the diagnosis process. The most common reasons of infertility-related stress were questions about the diagnosis from people in the neighborhood (75.0%), constantly having to go to the doctor (69.1%) and get permission from work during this process (22.1%) (Figure 1). Only women who experience infertility-related stress during the diagnosis process answered. At the same time, one person marked multiple options.
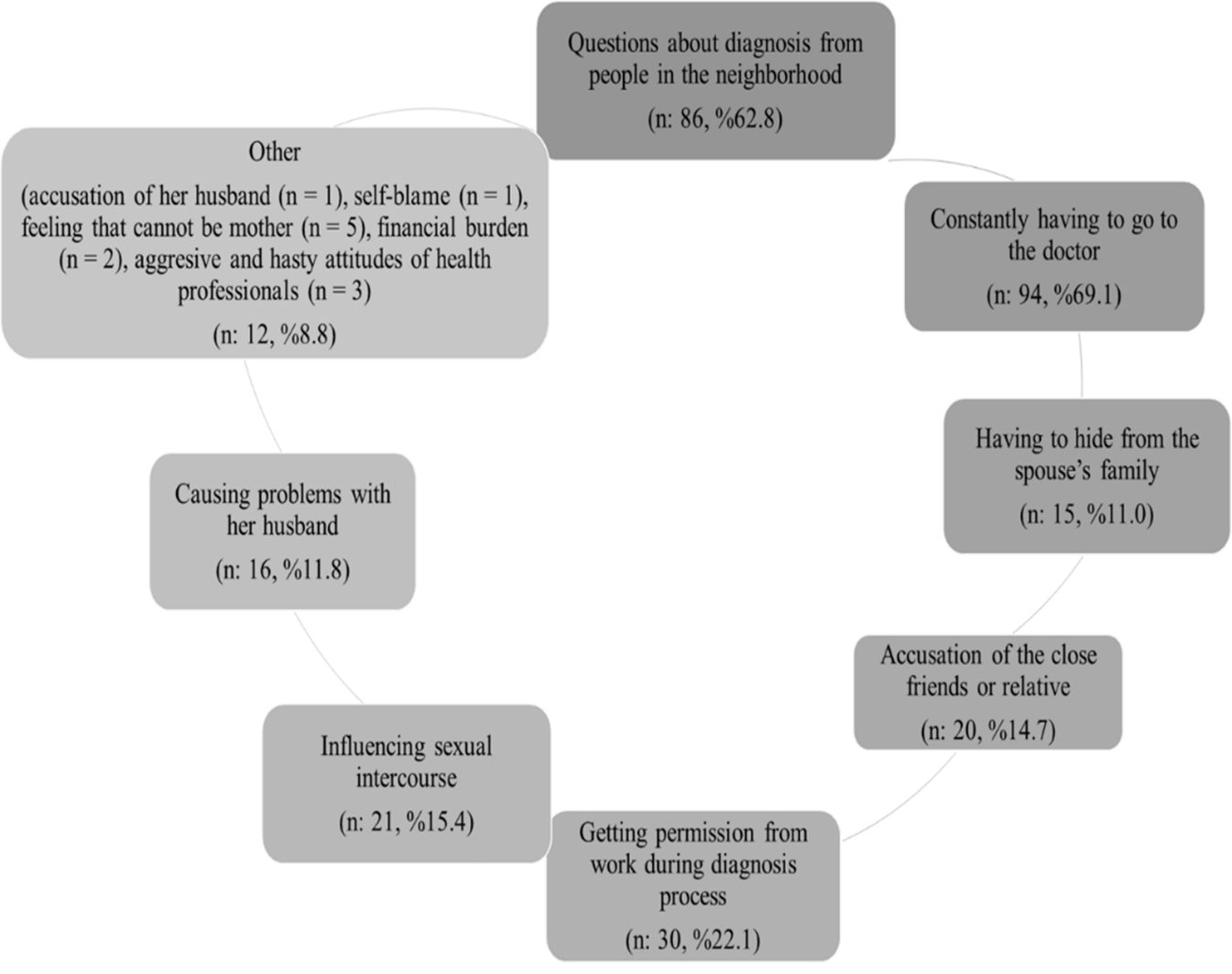
Figure 1: Reasons of infertility-related stress during the diagnosis process
It was determined that the most stressful time for women in the diagnosis process were when they expected test results related to the diagnosis (40.5 %), first learned about the diagnosis (27.2 %), on the control days (19.1 %) (Figure 2). Women experienced stress during the diagnosis answered.
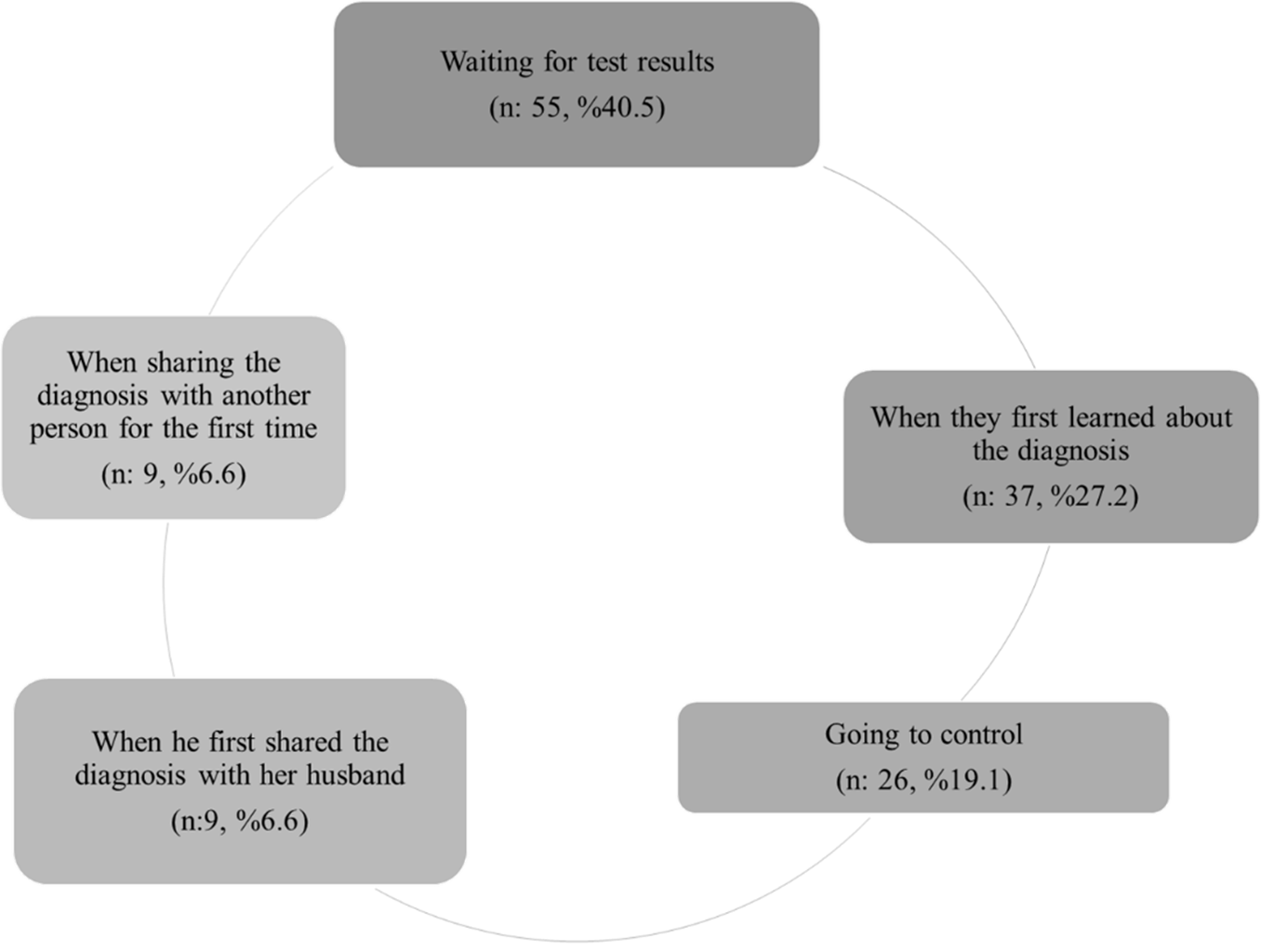
Figure 2: Socio-demographic and infertility characteristics (n: 154) The most stressful time during the diagnosis process
3.2.2. Reasons of the infertility-related stress and most stressful time during the treatment process
During the treatment process, 89.0 % (n: 137) of women stated that they experienced infertility-related stress. Questions from the people in the neighborhood related to treatment (62.8 %), going to the doctor (60.6%), and the probability of treatment failure (42.3 %) was included as the most frequent conditions that cause stress during the treatment process (Figure 3). Women who experience infertility-related stress during the diagnosis process answered. At the same time, one person marked multiple options.
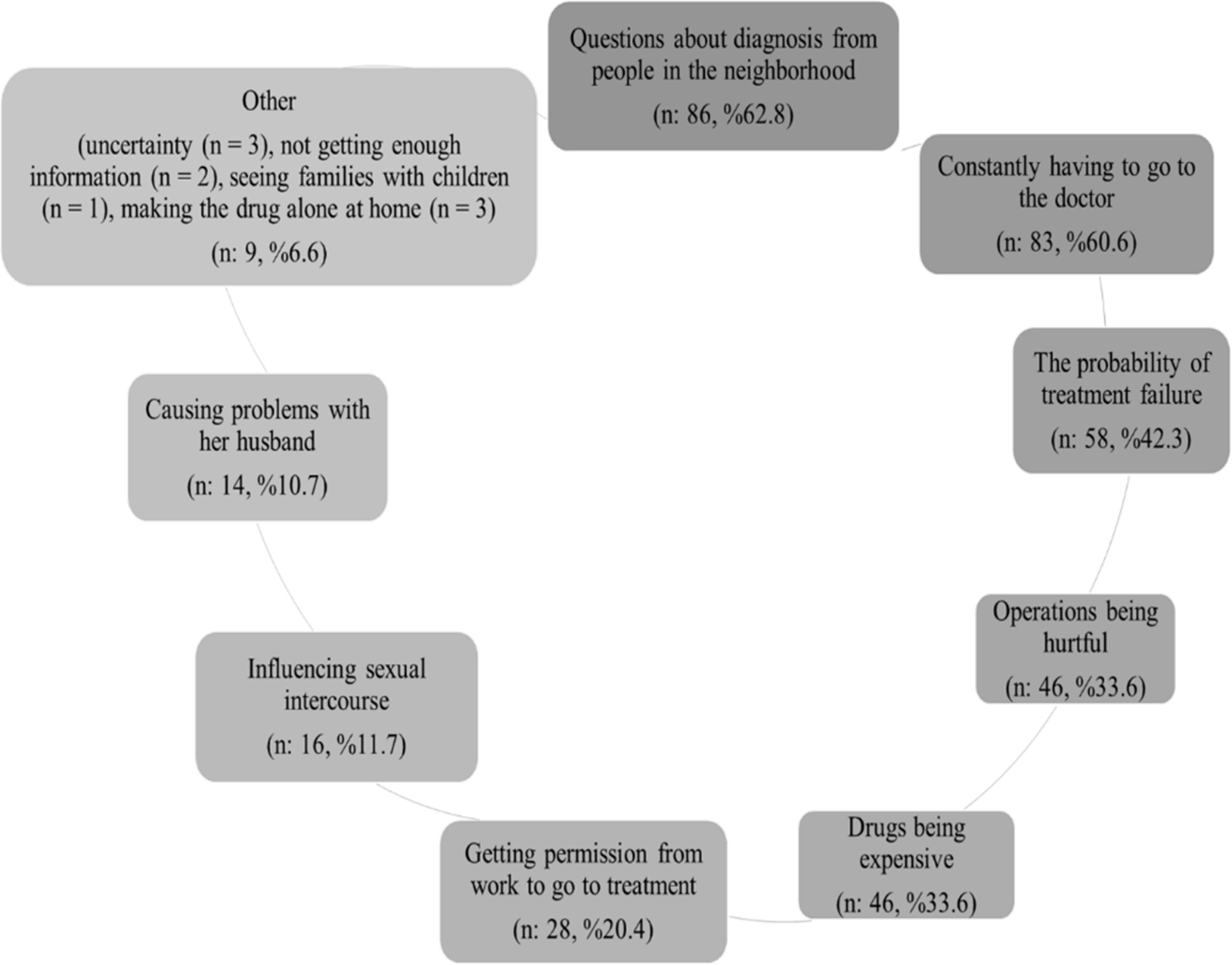
Figure 3. Reasons of infertility-related stress during the treatment process
When we look at the most stressful time experienced during the treatment process, it was seen that women experienced the most stress on embryo transfer day (27.7 %), on the first day of treatment (24.1 %) and OPU day (19.0 %) (Figure 4). Women who experienced stress during the treatment answered.
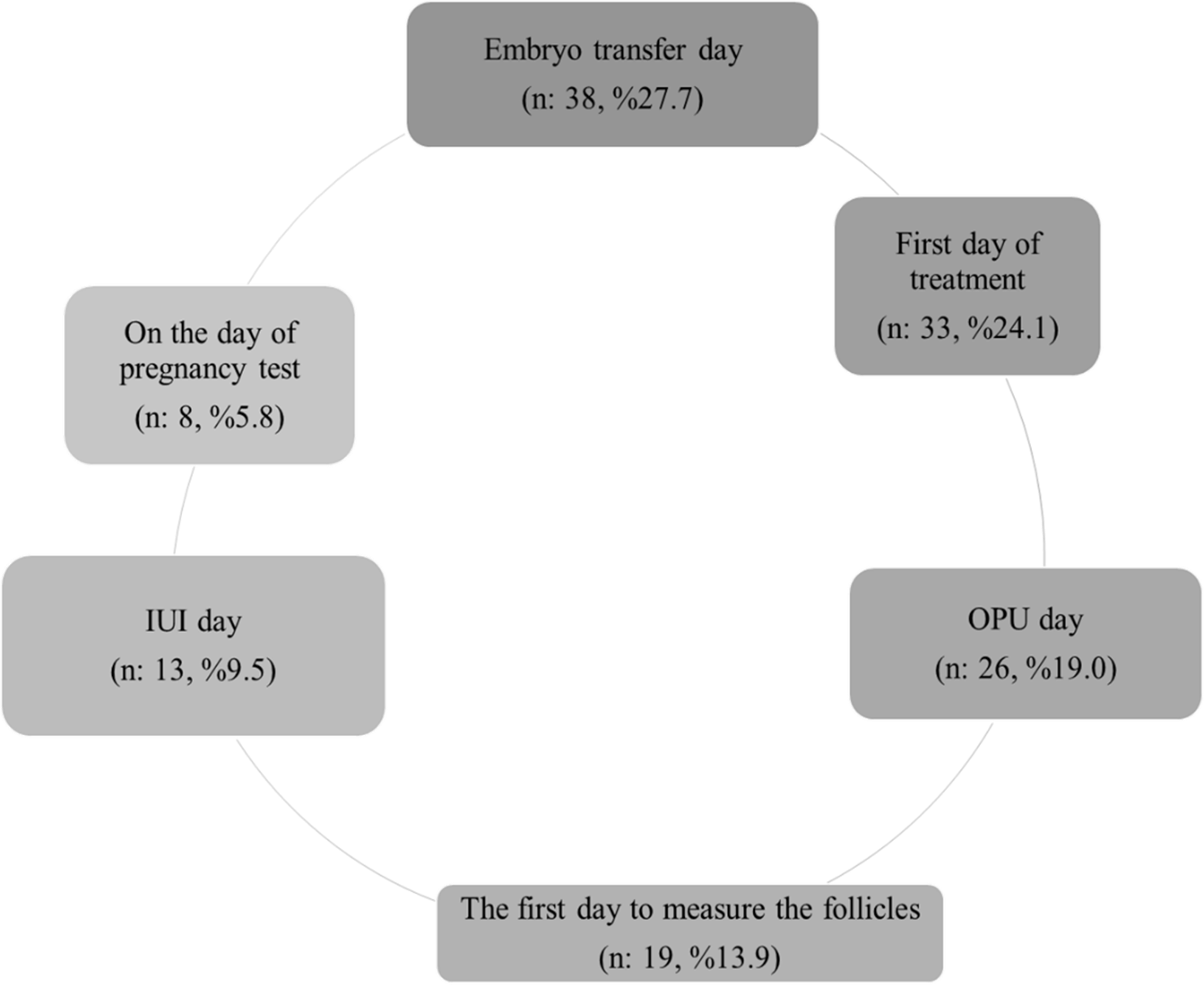
Figure 4. The most stressful time during the treatment process
Discussion
Both the diagnosis and the treatment process were stressful for women who received infertility treatment. In routine, the stress of women has not been seen as a problem and is not systematically evaluated in clinical practice. The study results highlight that the stress of the woman in the diagnosis and treatment process should be assessed and relaxation methods should be practiced to reduces stress. Reasons of the infertility-related stress and most the stressful time during the diagnosis process
It has been determined that the majority of women experience stress during the diagnosis of the infertility process. Karaca & Ünsal (2015) examined the stress levels of primary infertile women at the stage of diagnosis or treatment with the “Fertility Problem Inventory” and found that their stress levels were above the average value [2]. In our country, women impose infertility such as not being able to meet the maternal instinct, not being able to give birth, feeling abstracted from society, feeling emotionally deprived of child support, not assuming social roles such as the mother, pregnant women, maternity, mother-in-law, and self-worth [13]. These meanings imposed by women cause stress in women. Women in the study expressed that questions about the diagnosis from people in the neighborhood, have to go to the doctor constantly, get permission from work to go to the examination, have to hide from the husband’s family, being accused from husband and other people, affecting negatively the sexual relationship, have problems with the husband, self-accusation, feeling that they could never be mother, financial burden, and the aggressive and hasty attitudes of the healthcare professionals were causes of stress. In Karaca & Ünsal's (2015) study, one reason why women experience stress is not being a mother [2]. Similar to the study of Altuntuğ, Kızılırmak, Başer & Ege (2012) [10], it was found in the study of Kırca (2011) that stress in the infertility process was caused by economic reasons, pressure from the environment, and a sense of loss of productivity [11]. Some of the reasons identified in the study experienced stress were similar to literature in Turkey. This is thought to be due to the meaning Turkish women attribute to infertility. In addition to the stress causes in the literature, many other reasons have been identified. In addition to the source of the cause of stress such as the woman, her husband, and her environment, these study results show that healthcare professionals also cause stress to women during the diagnosis phase. They stated that their stress was the most intense when they were waiting for the test results, first got the diagnosis, went to the controls, shared the diagnosis with someone first, shared the diagnosis with their husband. In the literature, studies investigating the most intense stress periods specific to the infertility diagnosis process have not been found. It is important to determine the times of the most intense stress to support women at these times. This study contributes to the literature with these new results.
Reasons of the infertility-related stress and most stressful time during the treatment process
The majority of women stated that the treatment process was also stressful. In different studies conducted in our country and the world, it was found that women experience stress during the treatment process [2,14,15]. The questions about the treatment process, having to go to the doctor constantly, getting permission from work to go to treatment, operations being hurtful, the drugs being expensive, affecting negatively the sexual intercourse, the problems with her husband, uncertainty, lack of enough information, seeing families with children, performing the drug alone at home, and the probability of treatment failure was among the reasons for experiencing stress after starting the treatment. Similarly in the study of Xiaoli et al. (2016) [16], it was determined that infertile women who were treated had pain and discomfort in the treatment process, their sexual relations were negatively affected, they had financial burden, and they had trouble coming to the fertility center for treatment. The fact that infertility drugs are frequently used, most drugs are subcutaneous, and women are self-administered, the drugs are expensive, and that sexual intercourse is considered as a way to have only children is subject causes stress in women as in studies in the world [5]. In other studies, it also shown that infertile women most frequently experience stress during treatment operations and waiting test results [10,11]. Findings in the literature and study highlighted that women experience stress more intensely at similar times. These results show once again the importance of attempts to reduce stress at these times.
In the study, it was determined that the stress related to the treatment was intense on the first day of the treatment, on the first day on which the follicles will be measured, on the day of OPU, on the day of IUI, on the day of embryo transfer, on the day of pregnancy test. In a study by Hammarberg, Astbury & Baker (2001) [5], it has been identified that waiting for examination results, starting assisted reproduction treatment, oocyte collection, waiting for the result after embryo transfer and learning that the treatment is unsuccessful are particularly stressful.
Conclusion and recommendations: The results show us the importance of supporting infertile women both at diagnosis and treatment stages by nurses.
Reasons of the infertility-related stress and most the stressful time during diagnosis process
According to the results of the study, since the majority of women experience stress during the diagnosis phase, health professionals working in this field should develop appropriate interventions to comfort women. Considering the causes of stress and times of intense stress determined at the stage of diagnosis, nurses should;
· Take in-service training on appropriate initiatives to relax the individual,
· State the importance of supporting employees by informing their employers,
· Give women enough time and answer their questions,
· Make suggestions about sexual life,
· Inform women when preparing for diagnostic procedures, during and after treatment,
· Participate husband in the diagnosis process,
· Provide information about financial opportunities and state support,
· Perform applications such as relaxation music that can help reduce stress in clinics.
This can help both reduce stress, ease the diagnosis process, and believe that the woman is cared for by the healthcare staff during this difficult process.
Reasons of the infertility-related stress and most stressful time during the treatment process
Most women experience stress during the treatment phase. For the reasons in the treatment process and the most intense stress periods, nurses should.
· Contact the employer and ensure that women could get permission, because the treatment days cannot be changed,
· Prepare women for treatment procedures, should give information during and after the procedure,
· Ensure that they use social security to reduce the cost of drugs,
· Provide written drug information and illustrated brochures that can be used while making the drugs alone at home,
· Give information about her sexual life during the treatment process,
· Apply relaxation programs to women before the treatment procedures.
These interventions can help both reduce stress and positively affect treatment results.
Acknowledgments: None.
Conflict of Interest: None to declare.
Author contribution: All of the authors have contributed to the concept (SF, MAT), design of this study (SF, MAT), literature search (SF, NB), data collection and analysis (NB, BY), statistical analysis (SF, MAT), manuscript preparation (SF, MAT, NB), manuscript editing (SF, MAT) and manuscript review (SF, MAT).
Author Note: This study was presented as a poster presentation in 1st International and II National Gynecology and Maternal and Child Health Congress, 07-08 October 2016, Izmir.
References- Matthiesen SMS, Frederiksen Y, Ingerslev HJ, Zachariae R (2011) Stress, distress and outcome of assisted reproductive technology (art): a meta-analysis. Human Reproduction. 26(10): 2763-76.
- Karaca A, Ünsal G (2015) The stress level of ınfertile women due to ınfertility and affecting factors. Journal of Education And Research in Nursing 2015; 12(2): 129.
- Klonoff-Cohen H, Chu E, Natarajan L, Sieber W (2001) A prospective study of stress among women undergoing in vitro fertilization or gamete ıntrafallopia n transfer. Fertility And Sterility. 76(4): 675-687.
- Domar AD. Body/Mind connection. In: Işık AZ, Vicdan K (translate) Boston IVF Infertility hand book. Istanbul, Turkey: Nobel Medicine Book; 2008. pp. 178.
- Hammarberg K, Astbury J, Baker H (2001) Women’s experiences of IVF: a follow-up study. Human Reproduction. 16(2): 374-83.
- Morreale M, Balon R, Tancer M, Diamond M (2010) The ımpact of stress and psychosocial interventions on assisted reproductive technology outcome. Journal Of Sex & Marital Therapy. 37(1): 56-69.
- Olivius K, Friden B, Borg G, Bergh C (2004) Why do couples discontinue ın vitro fertilization treatment? a cohort study. Fertility and Sterility. 81(2): 258-261.
- Rajkhowa M, Mcconnell A, Thomas GE (2006) Reasons for discontinuation of ivf treatment: a questionnaire study. Human Reproduction. 21(2): 358-363.
- Coşkun AM. Family planning and infertility. In: Women's health and diseases nursing handbook. 2nd ed. Istanbul, Turkey: Koc University Press; 2016. pp.381.
- Altuntuğ K, Kızılırmak A, Başer M, Ege E. Anxiety level and sociodemographic characteristics in infertile couples. Fırat Health Services Journal 2012; 7(21): 65.
- Kırca N. Evaluation of psychosocial problems experienced in the treatment process of women successful in ınfertility treatment. Published Master Thesis, Atatürk University Institute of Health Sciences, Erzurum, 2011.
- Koçyiğit O. Infertility and socio-cultural effects. Journal Of Human Science 2012; 36.
- Sezgin H, Hocaoğlu Ç. Psychiatric aspect of infertility. Current Approaches in Psychiatry 2014; 6(2): 174.
- Gradvohl SMO, Osis MJD, Makuch MY (2013) Estresse de homense mulhere que buscam tratamento para infertilidade. Revista Brasileira De Ginecologia A Obstetricia. 35(6): 255-261.
- Miles L, Keitel M, Jackson M, Harris A, Licciardi F (2009) Predictors of distress in women being treated for ınfertility. Journal Of Reproductive And Infant Psychology. 27(3): 245-.
- Xiaoli S, Mei L, Junjun B, Shu D, Zhaolian W, et al. (2016) Assessing the quality of life of ınfertile chinese women: across-sectional study. Taiwanese Journal of Obstetrics & Gynecology. 55(2): 244-50.