


Drissia BENFADIL*, Lachakar AZZEDINE, Fahd EL IDRISSI EL AYOUBI
Department of Otorhinolaryngology and Head&neck Surgery, Oto-neuro-ophthalmology Research Laboratory (LRONO), University Hospital Mohamed 6, medicine faculty, University Mohammed I, Oujda, Morocco
*Corresponding Author: Drissia BENFADIL, Department of Otorhinolaryngology and Head&neck Surgery, Oto-neuro-ophthalmology Research Laboratory (LRONO), University Hospital Mohamed 6, medicine faculty, University Mohammed I, Oujda, Morocco.
Abstract
Thyroid tuberculosis is a rare localization, and a picture non-specifically makes the clinical symptomatology of goiter or complicated forms of thyroid tuberculosis.
The diagnosis is made after a histopathological examination on fine -needle aspiration or operative specimen after thyroidectomy.
Surgical treatment includes total thyroidectomy or drainage of an abscessed cervical and medical collection after diagnostic confirmation, based on the combination of three powerful antibiotics: rifampicin (R), isoniazid (H), and pyrazinamide (Z).
We report a case of thyroid tuberculosis aged 60 years old, complicated by cervical fistulization; the positive diagnosis is made after a percutaneous biopsy puncture of the mass and histopathological study. Anti-tuberculosis treatment was started for six months with a favorable clinical outcome.
Introduction
Thyroid tuberculosis is a rare form of extrapulmonary tuberculosis, even in endemic countries, and its discovery is usually accidental.it is a form that Lebert first described in 1862 [1]. Its frequency is estimated between 0.1-1 % in clinical series and 2-7 % in autopsy data [1].
The Clinical picture needs to be more specific, which makes diagnosis difficult. Our article aims to report a new case of this localization and discuss the diagnosis and therapeutic modalities.
Case Presentation
Our case concerns a 60-year-old patient with no notable pathological history, who consulted in our training for a median cervical swelling in pre-fistulization evolving for 1 and a half months, progressively increasing in volume, non-compressive and without signs of hypothyroidism, with thinning fever and moderate deterioration in general condition.
Cervical examination finds an anterior median basis-cervical mass above the sternal manubrium, ulcerated in pre-fistulization with local inflammatory signs (Figure 1). The remainder of the cervical exam finds no lymphadenopathy or other cervical mass. Nasofibroscopic examination shows no lesions associated with the larynx and pharynx, and the vocal cords were mobile.
A cervical ultrasound was performed: the objective of a multinodular goiter with probably a left inferior polar cystic nodule of the left lobe with blurred outlines and hyperechogenic echostructure.
Cervicothoracic CT, the objective cervical cystic mass of the anterior mediastinum in contact with the lower pole of the left thyroid lobe, and the chest x-ray is without abnormality (Figure 2 et 3).
The TSH level was average, and the rest of the biological workup was unremarkable.
Flexible bronchial microscopy found anthracosis spots, and a biopsy was done with bronchial aspiration showing necrotizing granulomatous tuberculoid inflammation suggestive of tuberculosis without signs of malignancy.
A percutaneous mass biopsy was performed with pathological examination objectifying the epithelioid and gigantocellular follicles with caseous necrosis, concluding in thyroid tuberculosis.
The patient received an anti-tuberculosis treatment based on: rifampicin (R), isoniazid (H), and pyrazinamide (Z) with good local progress.

Figure 1: an anterior median basis-cervical mass above the sternal manubrium, ulcerated in prefistulization with local inflammatory signs
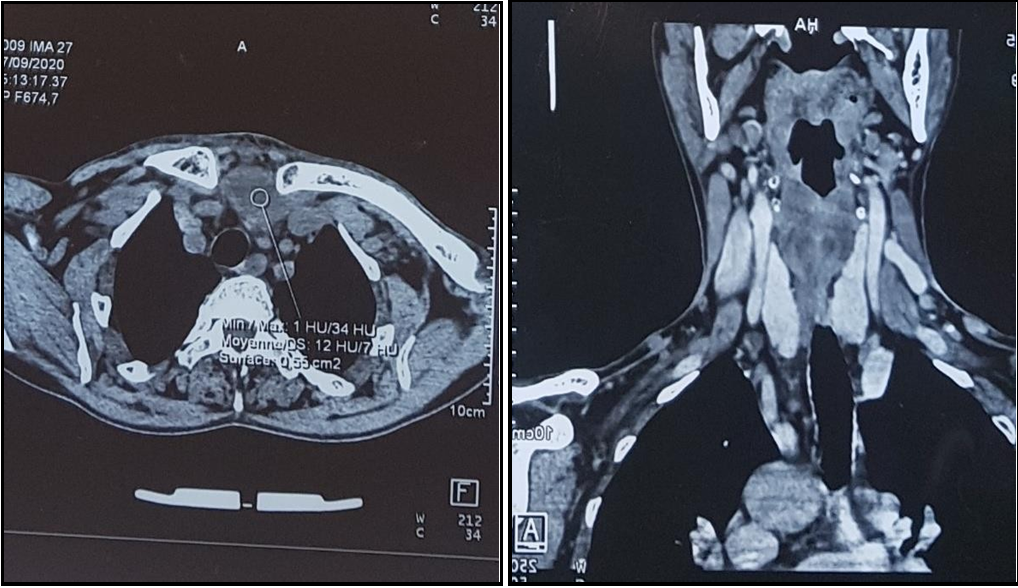
Figure 2 et 3: Cervico-thoracic CT, objective cervical cystic mass of the anterior mediastinum in contact with the lower pole of the left thyroid
Discussion
Described in the 19th century by Albers in 1862, thyroid tuberculosis is a rare form even in endemic areas (0.1 to 0.4 % of all locations).it occurs at any age with a predominance for the 20-29 age group and the female sex seems to be the most affected (70 to 80 % )which is consistent with the high frequency of thyroid disease in women [2]. From a pathogenetic point of view, there is a particular resistance of the thyroid body to tuberculosis infection by vascularization and the biostatic character of the thyroid hormones. But some factors sensitize the thyroid to bacillary disease, such as advanced age, diabetes, immunosuppression (AIDS), and malnutrition [3].
Diagnosis of thyroid tuberculosis remains difficult since no specific clinical presentation exists. However, several clinical aspects may reveal thyroid tuberculosis (anterior cervical swelling isolated or associated with satellite lymphadenopathy, modification of a pre- existing goiter with the appearance of pain or increase in volume, symptoms of thyroiditis .such as; fertilization in the skin as is the case for our patient or fistulization in a neighboring organ, hypothyroidism by the destruction of the gland, laryngotracheal, esophageal recurrent or even sympathetic compression. [4]. Sometimes, clinical symptoms may boil down to unexplained fever [3].
These clinical aspects can be associated with clinical or biological orientation elements, such as tuberculosis contagion, history of tuberculosis, skin fistula on clinical examination, associated fever, and inflammatory syndrome [5].
The differential diagnosis of this condition includes all other involvement of the thyroid gland.
For the assessment, a thyroid ultrasound is essential. It gives the characteristics of the nodule and the adjacent thyroid parenchyma (isolated nodule or nodular goiter) and provides information on the existence or not of lymphadenopathy [6].
In a cervical CT scan with an injection of the contrast product, the lesion will appear as an enhanced hypodensity on its periphery. The presence of cervical lymphadenopathy is possible [7].
The other additional examinations are only of interest to guide the diagnosis (TB skin test, CBC, and Sed rate) and to search for a second infectious site (x-ray of the lung, bacteriological analysis of expectorated sputum …).
The definitive positive diagnosis of thyroid tuberculosis can only be made on the histopathological examination of the surgical specimen, making it possible to rule out a neoplastic association [8].
Surgical treatment includes total thyroidectomy or drainage of a cervical abscess collection.
After a positive postoperative diagnosis, the treatment is primarily medical.it is based on the combination of three powerful antibiotics: rifampicin (R), isoniazid (H), and pyrazinamide (Z), according to the 2 RHZ/4 RH protocol. If the patient develops sequelae hypothyroidism, opotherapy should be prescribed based on TSH us levels.
The pathology course is often favorable without sequelae. The risk of relapse or non-cure despite a well-conducted treatment remains 1 % [8].
Conclusion
Tuberculosis of the thyroid is a rare condition. Its definitive diagnosis is, above all, histological. Its treatment is primarily medical based on a combination of antibiotics.
References
- Kabiri H, Atoini F, Zidane A (2007) La tuberculose thyroïdienne Thyroid tuberculosis. Annales d’Endocrinologie. 68(2-3): 196– 198.
- Ghosh A, Saha S, Bhattacharya B, Chattopadhay S (2007) Primary tuberculosis of thyroid gland: a rare case report. American J Otolaryngol 28(4): 267-70.
- Garg SK, Ganapathy V, Bandhopadhya PK, Gupta SK, Dash RJ (1987) Pyrexia of unknown origine as rare presentation of tuberculosis thyroiditis. Indian J Chest Dis Allied Sci. 29(1): 52– 5.
- Moumen M, Touhami M, EL Fares F, Benchakroun Y (1992) LA TUBERCULOSE THYROIDIENNE A PROPOS DE 3 CAS. Médecine du Maghreb.
- Thyroid tuberculosis H. Kabiri*, F. Atoini, A. Zidane Department of thoracic surgery, Mohamed -V military training hospital, May 29,2007 Annals of Endocrinology 68 (2007) 196–198).
- National Agency for Accreditation and Health Evaluation. Recommendation for clinical practice: diagnostic management of the thyroid nodule .surgery ann 1996;50:555–64.
- Andrius S (2004) Thyroid tuberculosis. Medicina (B Aires). 40(3): 201–204.
- Chaulet P, Boulahbal F (1995) clinical trial of a fixed ratio combination of three drugs in the treatment of tuberculosis. Tuberculosis Chemotherapy Task force. Tuber Lung Dis. 76(5): 407–12.