


Dr. Venkatesh Gupta S.K¹, *, Animesh Yadav², Jayanth B²
1Department of Orthopedics JJMMC Davangere, Karnataka, India
*Corresponding Author: Venkatesh Gupta S.K, Department of Orthopedics JJMMC Davangere, Karnataka, India
Abstract
Pyle metaphyseal dysplasia is an infrequent autosomal recessive skeletal disorder affecting the metaphysis of long tubular bones. A 13-year-old girl with Pyle’s disease presented with mild facial dysmorphism, deformity of the bilateral upper limb, cubitus valgus, and genu valgum. Her Skeletal radiology showed the distinctive Erlenmeyer flask sign at distal femoral and proximal tibia metaphyses along with an old pathological fracture of the left humerus with exuberant callus and minimal platyspondylosis.
Keywords: pyle’s disease, metaphyseal dysplasia, erlenmeyer flask sign
Introduction
Metaphyseal Dysplasia also called Pyle’s disease is an autosomal recessive disorder that manifests at a variable age. Edwin Pyle American orthopedics in 1931 described this disorder first in a five- year-old child [1]. Patients present with benign clinical symptoms and signs which include joint pain muscular weakness, scoliosis, pathological fractures, wrist swelling, genu valgum, limited extension of the elbow, dental malocclusion, and bone fragility [2]. Distinct expansion of the metaphyseal segments of tubular leads to an "Erlenmeyer flask sign" appearance on radiography peculiarly in the distal femur and proximal tibia. A total of 35 cases of Pyle’s disease have been reported to date [3].
Case Report
A 13-year-old female child was referred to Department of Orthopedics, JJM Medical College, Davangere, India for assessment of deformity in both upper limbs from Bapuji dental college and hospital. She presented with a deformity in both upper limbs for 2 years.Patient’ father gives history of fracture of right arm after trivial trauma 2 years back treated with POP slab and later reassured regarding the deformity. There was no developmental delay and gross motor milestones were achieved as per age without any bone or joint pain. There is history of jaundice at birth and she was admitted for 3 weeks in NICU for the same. There is a third-degree consanguinity andthere was no family history of similar problem. On general physical examination the child weight was 26 kilograms with the height of 112 centimeters. She had multiple impacted teeth with eruption cyst and reactive osteitis of mandible. She also had anterior bowing ofboth humerus and swelling of the proximal humerus (Figure. 1), lateral bowing of both bones of the forearm with the widening of the wrist along with cubitus valgus and genu valgum [5]. The central nervous system, motor, sensory and reflexes examinations were normal with no limb length discrepancy. Spine and other joints examination was normal. Blood investigation and ultrasound abdomen were within normal limits [6]. Skeletal survey showed metaphyseal flaringand thinning of cortices and ground-glass opacity of matrix in bilateral distal femur (Figure. 2) and proximal tibiae suggestive of Erlenmeyer flask deformity with smoke up the chimney appearance and enlarged neck of femur (Figure. 3). Old pathological fracture at left proximal humerus with exuberant callus and bone remodeling defect (Figure. 4). Mild expansion of distal end of radius and ulna with bowing of both bones and cubitus valgum (Figure. 5). X-ray of Thoraco-lumbar spine shows diffuse osteopenia and minimal platyspondylosis was also seen (Figure. 6). X-ray skull shows misaligned teeth (Figure. 7) and ribs also appeared widened on X-ray chest. Based on clinical features and radiological findings, we made a diagnosis of Pyle’s metaphyseal dysplasia [2].

Figure. 1 Anterior bowing of both humerus and swelling of proximal humerus

Figure. 2 Widening and thinning of cortices and ground glass opacity of osteoid matrix in bilateral distal femur suggestive of Erlenmeyer flask deformity with enlarged neck of femur [4].

Figure. 3 Widening and thinning of cortices and ground glass opacity of osteoid matrix in bilateral proximal tibia suggestive of Erlenmeyer flask deformity.

Figure. 4 Old pathological fracture at left proximal humerus with exuberant callus and bone remodeling defect.
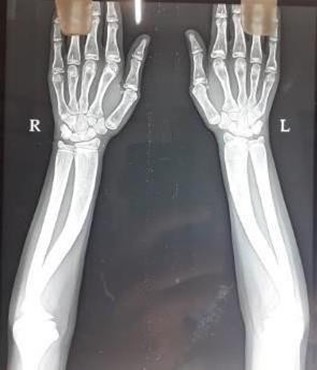
Figure. 5 Mild expansion of distal end of radius and ulna with bowing of both bones and cubitus valgum

Figure. 6 diffuse osteopenia and minimal platyspondylosis.

Figure. 7 sclerotic skulls with overcrowded impacted teeth [7].
Discussion
Till now globally 35 cases reported. The foremost case was reported by Edwin Pyle in 1931 [1]. He presented a 5- year- old child with skull and limb deformities. The patient had prominent painless knock knee deformity, long bones of arms and legs were enlarged at the ends. He suggested it as a failure of bone resorption as the pathophysiological basis of disease, which would lead to the superimposition of several layers of under modeled bone at the metaphysis.
Bakwin and Krida reported familial incidence in 1937 and by Hermal et al in 1953. Heselson et al described the radiological features of Pyle’s disease in 1979 i.e., thinning of cortices in areas of bony expansion [4]. The etiology has however still not been made whether it is familial or because of consanguinity. Pyle's metaphyseal dysplasia is an uncommon autosomal recessive skeletal dysplasia with the causative SFRP4 gene [8]. Clinical signs and symptoms are benign which includes joint pain, muscular weakness, scoliosis, pathological fractures, genu valgum, limited extension of the elbow, dental malocclusion, and bone fragility [9]. In this patient she had anterior bowing of both humerus, cubitus valgus, widening of the wrist, genu valgum, overcrowding of teeth with normal physical and mental development. The upper extremity was more affected than lower in our case.
Pyle’s disease has distinctive radiological findings characterized by extensively widen metaphyses of the distal end of the femur and proximal tibia with marked cortical thinning and osteoporosis (Erlenmeyer-flask deformity) [10]. Proximal two-thirds of the humerus and distal two-thirds of radius and ulna may show similar changes. Similar but fewer changes may be observed in other long bones, metacarpals, and phalanges. Moderate platyspondylosis to biconcave lens appearance of the vertebral bodies noticed in the spine. Skeletal survey of our patient revealed widening of the metaphysis and thinning of cortices (Erlenmeyer flask sign) in long bones with a pathological fracture at left proximal humerus with exuberant callus and bone remodeling defect. and mild platyspondylosis. In reported cases of Pyle’s disease, these appearances are consistent. Patients may also present with dental caries, mandibular prognathism, multiple retained deciduous teeth and crowding of teeth. Our patient also has overcrowded impacted teeth [7]. The pathophysiology of Pyle’s disease is adequately understood. But it is probably due to the subperiosteal remodeling failure in the metaphyses [11]. Chronic hyperaemia of the perichondral ring of osteoblasts may be the cause for remodeling failure. Congenital hyperplasis of the perichondral ring arteries may be the cause for hyperaemia. The differential diagnosis for Erlenmeyer flask deformity is lysosomal storage diseases (Gaucher disease) and Niemann Pick type B, hemoglobinopathies (thalassemia, sickle cell disease membranous lipodystrophies, craniodiaphyseal dysplasia, osteopetrosis, Braun Tinschert dysplasia [12]. And the absence of typical changes in laboratory tests and characteristic clinical manifestations rules out the possibility of hematological as well as storage disorder in our patient. Diagnosis of Pyle’s disease is done through clinical evaluation, imaging, and gene sequence analysis for the entire coding region or deletion duplication analysis of SFRP4 gene. As the patient was having normal gait and no limitation of routine activities the patient was managed with physiotherapy (strengthening exercise) and later deciduous tooth extraction for the impacted tooth.
References
- Pyle E (1931) A Case of Unusual Bone Development. Journal of Bone and Joint Surgery 13(4): 874-876.
- Percin EF, Percin S, Koptagel E, Demirel H (2003) A case with Pyle type metaphyseal dysplasia: clinical, radiological and histological evaluation. Genet Couns 14(4): 387-393.
- Raad MS, Beighton P (1978) Autosomal recessive inheritance of metaphyseal dysplasia (Pyle disease). Clin Genet 14(5): 251- 256.
- Heselson NG, Raad MS, Hamersma H, Cremin BJ, Beighton P (1979) The radiological manifestations of metaphyseal dysplasia (Pyle disease). Br J Radiol 52(618): 431-440.
- Gupta N, Kabra M, Das CJ, Gupta AK (2008) Pyle metaphyseal dysplasia. Indian Pediatr 45: 323-325.
- Turra S, Gigante C, Pavanini G, Bardi C (2000) Spinal
- involvement in Pyle’s disease. Pediatr Radiol; 30(1): 25-27.
- Narayananan VS, Ashok L, Mamatha GP, Rajeshwari A, Prasad SS (2006) Pyle’s disease: an incidental finding in a routine dental patient. Dentomaxillofac Radiol 35(1): 50-54.
- Lindberg EJ, Watts HG (1997) Postosteotomy healing in Pyle’s disease (familial metaphyseal dysplasia). A case reports. Clin Orthop Relat Res 1997; 341: 215-217.
- Ferrari D, Magnani M, Donzelli O (2005) Pyle’s disease.A description of two clinical cases and a review of the literature. Chir Organi Mov 90(3): 303-307.
- David JEA, Palmer PES, Bulawayo, Rhodesia S (1958) Familial Metaphysial Dysplasia. The Journal of Bone and Joint Surgery 40(1): 86-93.
- Khanal D (2016) Metaphyseal Dysplasia: A Rare Case Report. J Clin Case Rep 6(2) Beighton P (1987) Pyle disease (metaphyseal dysplasia). J Med Genet 24(6): 321-324.