


Dr. Qasim Abbas*, Dr. Said Al Busafi, Dr. Khalid Al Shamousi, Dr. Ahmed Al Wasssief, Dr. Leena Balla
Department of Internal Medicine, GI-unit, Sultan Qaboos University Hospital, Muscat, Oman.
*Corresponding Author: Dr. Qasim Abbas, Department of Internal Medicine, GI-unit, Sultan Qaboos University Hospital, Muscat, Oman
Introduction
Background:
Gallstone-related diseases are common in western countries. Based on ultrasound studies, the prevalence of gall stones is more than 10% in the USA and European countries [1]. Cholecystitis was among the top 20 causes of GI-related deaths [2]. The prevalence of gallstones appears to be rising due to the epidemic of obesity associated with insulin resistance and metabolic syndrome. Each year, roughly 1 million new cases are discovered [3,4,5].
Although many gallstones are silent, about one-third eventually cause symptoms and complications [6].
Laparoscopic cholecystectomy (LC) is the technique of choice for managing the patient with biliary pain and complications of gallstones. It is associated with fewer complications and shorter hospital stays than open cholecystectomies [7].
One of the complications of cholecystectomy is the migration of surgical clips into the common bile duct (CBD), albeit very rare [8]. Migration of the surgical clip into the CBD can lead to biliary stone formation and obstruction, and the patient can present with biliary colic, cholangitis, or pancreatitis over a variable period. The exact pathophysiological process of clip migration is not fully understood, but it is thought to be related to cystic stump necrosis and movement of the clip to a low-pressure system via the CBD [9]. The risk factors for clip migration include previous complicated gallstone disease, inaccurate clip placement, and distorted anatomy [8].
Here we present a case of pancreatitis caused by a stone formed around a migrated surgical clip into CBD four years after laparoscopic cholecystectomy.
Case Summary
A 50-year-old Omani woman presented to the Emergency Department with a five-week history of abdominal pain described as colicky, non-radiating, and recurrent in nature and mainly appreciated over the epigastric area and right upper quadrant. The pain was associated with nausea but not specific aggravating and relieving factors. There was no associated fever, vomiting, jaundice, or change in urine color. The pain worsened in the 24 hours preceding presentation to the emergency department and was more constant.
History divulged a medical background of hypertension, hypothyroidism, and a history of laparoscopic cholecystectomy done 4 years earlier. Her regular medications included levothyroxine 25 mcg OD, amlodipine 10 mg OD, and valsartan 80 mg OD. She had no significant family history of allergy to medicines. She was not a smoker or ethanol consumer.
Physical examination: On presentation, the patient was alert and conscious with a temperature of 36.3, heart rate of 88 beats/minute, respiratory rate of 18 breaths/minute, a saturation of 96 % on room air, and BP of 168/88 mmHg.
The abdominal examination revealed mild epigastric tenderness, while the systemic examination was unremarkable.
Investigations: Hb 12.1 g/dL, WCC 7.700/mol, PLT 253/L, ALT 667 U/L, ALP 299 U/L, AST 622 U/L, Bilirubin 19 mmoL/L, lipase 2839 U/L, LDH 577 U/L, CRP 7 mg/dL. Normal calcium, phosphate, renal function tests, troponin, and INR.
The abdominal US reported a mildly enlarged liver (measuring ~15 cm in size) with slightly coarse echotexture and smooth margins. Status post cholecystectomy was confirmed with the non- visualization of her gallbladder. No intrahepatic biliary ductal dilatation was seen, but CBD was mildly dilated, measuring about 7 mm in diameter. No distal obstructive stone or lesion could be identified. The pancreas is obscured by bowel gases and cannot be visualized.
The patient was admitted with the impression of biliary pancreatitis and received standard management of generous intravenous hydration and analgesia.
Inpatient Progress: A subsequent CT abdomen during admission reported that the liver was normal in size and enhancement pattern with no focal lesions. A small metallic clip was seen at the inferior aspect of the right lobe of the liver. Status post cholecystectomy confirmed further by the absent gallbladder. No intrahepatic biliary ductal dilatation was seen. The common bile duct was dilated, measuring approximately 11 mm in diameter, with a small? A metallic structure was seen at the distal aspect of the CBD, which was suspected to be a migrated cholecystectomy clip (Figure 1, 2). The pancreas looks normal.

Figure 1: Computed tomography image showing the common bile and surgical clip (arrow).
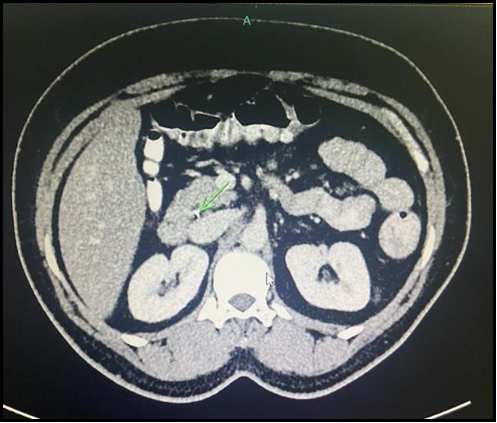
Figure 2: Computed tomography image showing the common bile and surgical clip (arrow).
Endoscopic retrograde cholangiopancreatography (ERCP) was performed, and a cholangiogram showed a mildly dilated CBD with a distal filling defect representing a stone (figure 3). Adequate endoscopic sphincterotomy was achieved, followed by extraction balloon sweeping, and a single stone was successfully removed from the CBD. This stone appeared to have formed around the migrated post-cholecystectomy surgical clip (Figure 4). Significant clinical and symptomatic improvement was demonstrated following the procedure, depicted by the eventual normalization of liver function tests. The patient was subsequently discharged from the hospital in a fit state.
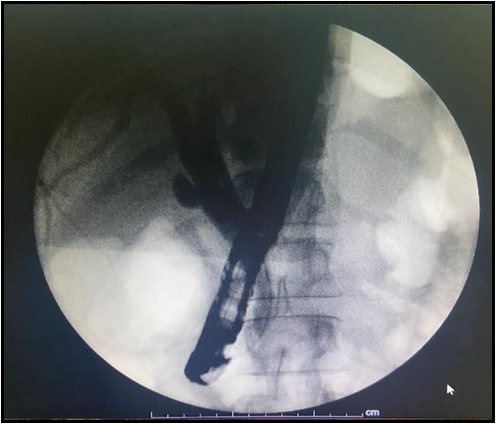
Figure 3: Endoscopic retrograde cholangiopancreatography showing a filling defect in the common bile duct.
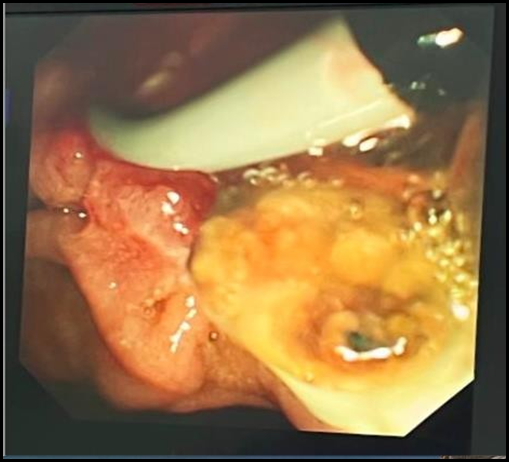
Figure 4: Endoscopic retrograde cholangiopancreatography luminal image of the stone surrounding the surgical clip.
Discussion
Migration of the surgical clip into the CBD is a rare complication that can lead to the biliary stone formation by acting as a nidus for stone formation [10].
The time of clip migration can vary from 11 days to 20 years, while the median time of migration is usually 2 years [8].
The exact pathophysiological process of clip migration is not fully understood, but it is thought to be related to cystic stump necrosis and movement of the clip to a low-pressure system via the CBD [9]. The risk factors for clip migration include previous complicated gallstone disease, inaccurate clip placement, and distorted anatomy [8].
The clinical presentation of stones formed due to clip migration is similar to non-iatrogenic stones, and the patient can present with biliary colic, cholangitis, or pancreatitis (as in our case) over a variable period.
ERCP is the first approach for treating clip migration, with a success rate of almost 85 %, while surgery should be reserved for unsuccessful procedures [11,12].
Conclusion
In conclusion, surgical clip migration into CBD is a rare complication of LC. It should be considered in the differential diagnosis while treating patients with a surgical history of LC. Early diagnosis and successful management of this complication can prevent serious complications.
Conflicts of Interest: The authors declare that there are no conflicts of interest regarding the publication of this article.
Authors’ Contributions: All authors contributed to manuscript preparation, reading, manuscript editing, manuscript review, and literature search.
References
- Kratzer W, Mason RA, Kachele V (1999) Prevalence of gallstones in sonographic surveys worldwide. J Clin Ultrasound. 27(1): 1-7.
- Russo MW, Wei JT, Thiny MT, Gangarosa LM, Brown A, et al. (2004) Digestive and liver diseases statistics, 2004. Gastroenterology. 126: 1448-53.
- Everhart J (2001) Gallstones and ethnicity in the Americas. J Assoc Acad Minor Phys. 12(3): 137– 43.
- Everhart JE, Khare M, Hill M, Maurer KR (1999) Prevalence and ethnic differences in gallbladder disease in the United States. Gastroenterology. 117(3): 632–9.
- Sandler RS, Everhart JE, Donowitz M, Adams E, Cronin K, et al. (2002) The burden of selected digestive diseases in the United States. Gastroenterology. 122(5): 1500–11.
- Diehl AK (1991) Epidemiology and natural history of gallstone disease. Gastroenterol Clin North Am. 20(1): 1-19.
- Holohan TV (1991) Laparoscopic cholecystectomy. The Lancet. 338(8770): 801–803.
- Chong VH, Chong CF (2010) Biliary complications secondary to post-cholecystectomy clip migration: a review of 69 cases. J Gastrointest Surg. 14(4): 688–696.
- Chong VH, Yim HB, Lim CC (2004) Clip-induced biliary stone. Singapore Med J. 45(11): 533–5.
- Li Q, Tao L, Wu X, Mou L, Sun X, et al. (2016) Bile duct stone formation around a prolene suture after cholangioenterostomy. Pak J Med Sci. 32(1): 263–266.
- Sheffer D, Gal O, Ovadia B, Kopelman Y (2020) Cholangitis caused by surgical clip migration into the common bile duct: a rare complication of a daily practice, BMJ Case Rep. 13(1): e231201.
- Onghena T, Vereecken L, Van den Dwey K, Van Loon C (1992) Common bile duct foreign body: an unusual case, Surg. Laparosc. Endosc. 2(1): 8–10.