


Abat Sahlu Baleh1, Abdulaziz Abdellah Hussein2*, Murtii Teressa Obolu3
1MD, Consultant Neurosurgeon, Associate Professor of Neurosurgery, Department of Surgery, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia
2MD, Consultant Neurosurgeon, Assistant Professor of Neurosurgery, Department of Surgery College of Medicine & Health Science, Hawassa University, Hawassa, Ethiopia
3MD, Senior Resident, Chief General Surgery Resident, Department of Surgery College of Medicine & Health Science Hawassa University, Hawassa, Ethiopia
*Corresponding Author: Abdulaziz Abdellah Hussein, MD, Consultant Neurosurgeon, Assistant Professor of Neurosurgery, Department of Surgery College of Medicine & Health Science, Hawassa University, Hawassa, Ethiopia.
Abstract
Background
Hemangioblastomas are highly vascular benign neoplasms predominantly affecting adults. It typically occurs in the central nervous system (CNS) predominantly in cerebellum, brainstem, and spinal cord and occasionally in cerebrum and extra neural tissues. In comparison to cerebellar hemangioblastoma; cases of brainstem hemangioblastomas are less common and those completely embedded within the parenchyma (intramedullary type) of the brainstem are very rare with only few cases reported in the literature.
Case presentation
We report a case of a 38-year-old female presented with worsening of headache, failure to maintain balance and right-side body weakness of one week duration, who was diagnosed to have intramedullary hemangioblastoma of the brainstem and was managed successfully. Here we report the findings in detail along with the results of 6 months follow-up.
Result
After correcting the hyponatremia and clinical stabilization, she was prepared for elective surgery. Patient was positioned prone, head fixed with 3-point head holder. Sub occipital craniectomy and C1 laminectomy was done. Dura was opened in Y-shape fashion and tucked up to the sub occipital muscles leaving the arachnoid intact. Under operating microscope, the right-side pia was opened. There was cherry red, highly vascular tumour found to be embedded in to the dorsal medulla. The tumour was then dissected from brain tissue and gently retracted. The ventral feeding arteries were identified, coagulated with bipolar forceps and divided. The tumour was completely excised and satisfactory postoperative outcome.
Conclusion
En block removal of such tumors reduces the complications and improves the outcome of the patients. Therefore; By increasing the availability of advanced neuroimaging and with improved microsurgical techniques, complete and safe resection of rare and difficult brain lesions like brainstem hemangioblastomas is possible in resource limited setups.
Keywords: Intramedullary hemangioblastoma, brainstem, medulla oblongata, forth ventricle
Introduction
Hemangioblastomas are highly vascular benign tumors (World Health Organization Grade I) of the central nervous system. They occur sporadically or in the autosomal dominant neoplasia syndrome, Von Hippel-Lindau (VHL) disease [1]. It accounts 2% to 3% of all brain tumors and the cerebellum is the most common site. Brainstem is involved less commonly [2, 3]. Brainstem hemangioblastoma can occur in three locations in relation to fourth ventricle: I) Type A - those tumors attached to the floor of the fourth ventricle II) Type E - those tumors partially embedded in the dorsal medulla oblongata and III) Type I - intramedullary. Patients with intramedullary hemangioblastomas commonly present with features of raised ICP, ataxic gait and bulbar signs [4]. Safe en block resection of the lesion and intensive postoperative care are the main stay of management to improve the outcome [4, 5]. Here we report a case of intramedullary hemangioblastoma of the brainstem with peritumoral cyst with a typical clinical and radiologic feature of intramedullary hemangioblastoma of the brainstem, which was managed surgically with good outcome.
Case presentations
History and physical examination
A 38-year-old woman presented with headache of 3 years duration which worsened over 3 weeks prior to her presentation. Associated with worsening of headache she was also complaining reduced appetite, nausea and vomiting of ingested matter, failure to maintain balance and right-side body weakness of 1 week duration.
On physical examination, GCS was 15/15 and cranial nerves were intact. Power was 4/5 on right side both in upper and lower extremities. Position and vibration sensation were reduced on right side and cerebellar signs were positive.
Investigations
Blood investigation revealed hyponatremia (Na+=122mg/dl), otherwise other results were within normal range. Magnetic resonance imaging (MRI) of brain showed a cystic (23mm x 28mm x 20mm) mass lesion with a mural nodule (8mm) which was hypointense on T1W images and hyperintense on T2W images with the vivid enhancement of the mural nodule with gadolinium contrast, occupying the caudal part of the fourth ventricle and the dorsal medulla predominantly on the right side. The caudal medulla was displaced ventrally and the vermis was displaced dorsally and superiorly with mild peritumoral edema (Figures 1-2). Whole neuro- axis MRI and abdominal ultrasound revealed no features of VHL.
Management outcome and follow ups
After correcting the hyponatremia and clinical stabilization, she was prepared for elective surgery. Patient was positioned prone, head fixed with 3-point head holder. Sub occipital craniectomy and C1 laminectomy was done. Dura was opened in Y-shape fashion and tucked up to the sub occipital muscles leaving the arachnoid intact. There was posterior bulge on right side of medulla oblongata with abnormal appearing veins on the surface.
Under operating microscope, the right-side pia was opened. There was a cherry red, highly vascular tumor found to be embedded into the dorsal medulla. Tumor was then dissected from brain tissue and gently retracted. The ventral feeding arteries were identified, coagulated with bipolar forceps and divided. A cleavage plane between the tumor and brain tissue formed by gliotic tissue was identified. The tumor was gently rolled back and forth with bipolar coagulation to reduce the size and finally it was removed en block. There was oozing blood from the tumor bed which was controlled easily with surgical and cottoned packing.
After securing hemostasis, dura was closed in water tight fashion using the pericranial tissue as a graft. Muscle, fascia and skin were closed layer by layer.
Postoperatively the patient was fully conscious and extubated with her vital signs being stable. The patient transferred to the ICU and the postoperative course was uncomplicated except slight worsening of right-side body weakness. She was discharged home at 4th postoperative day. On discharge, the right-side power was 3/5 in upper extremity and 4/5 on lower extremity with vibration and position sensations lost on same side.
Early postoperative head CT with contrast and post-contrast MRI at 6 months after surgery demonstrated no residual tumor with expected postoperative changes (Figure 3). The pathologic analysis confirmed it to be hemangioblastoma (WHO grade one) (figure 4). During her follow up, she was having progressive improvement. The difficulty in maintaining balance and the right-side body weakness improved progressively. At 6th months follow up the power on the right side was 4+/5 and both position and vibration sensation were fully recovered.
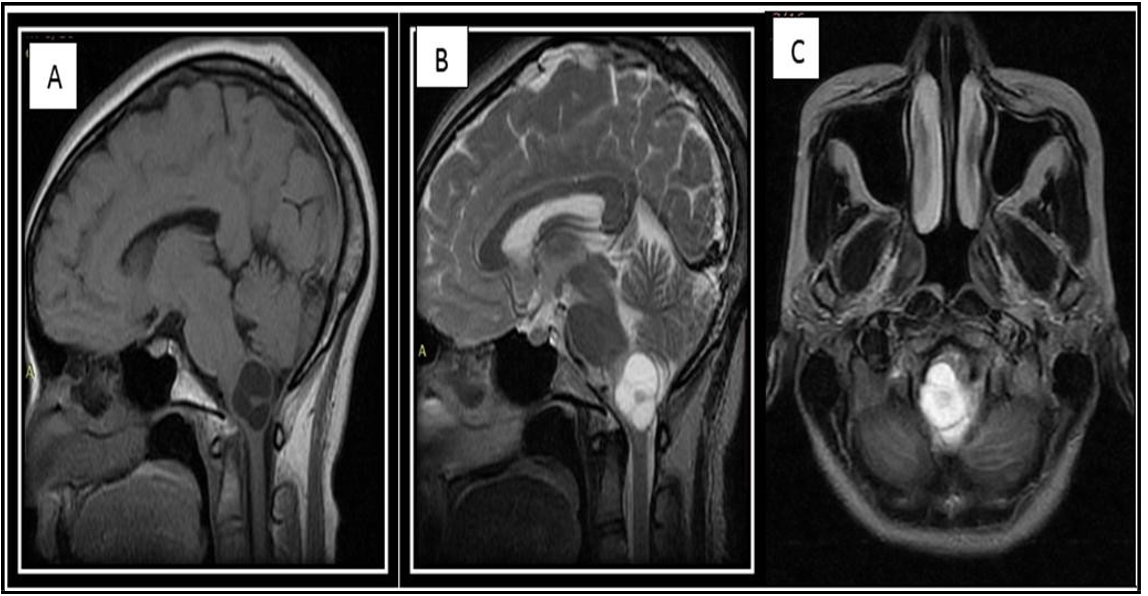
Figure 1: Preoperative MRI T1W sagittal (A),T2W sagittal (B) and axial T2W (C) images showed well defined cystic mass with mural nodule in the caudal part of fourth ventricle and dorsal medulla more on right side
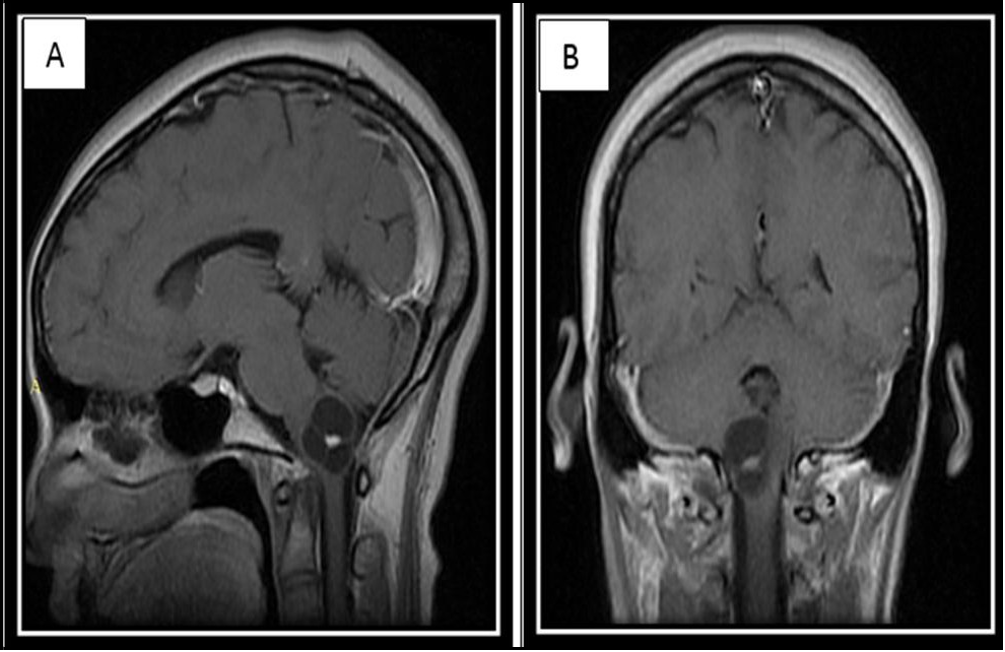
Figure 2: Preoperative MRI with gadolinium contrast T1W sagittal and coronal (A, B) showed vivid enhancement of the mural nodule with no enhancement of the cystic wall
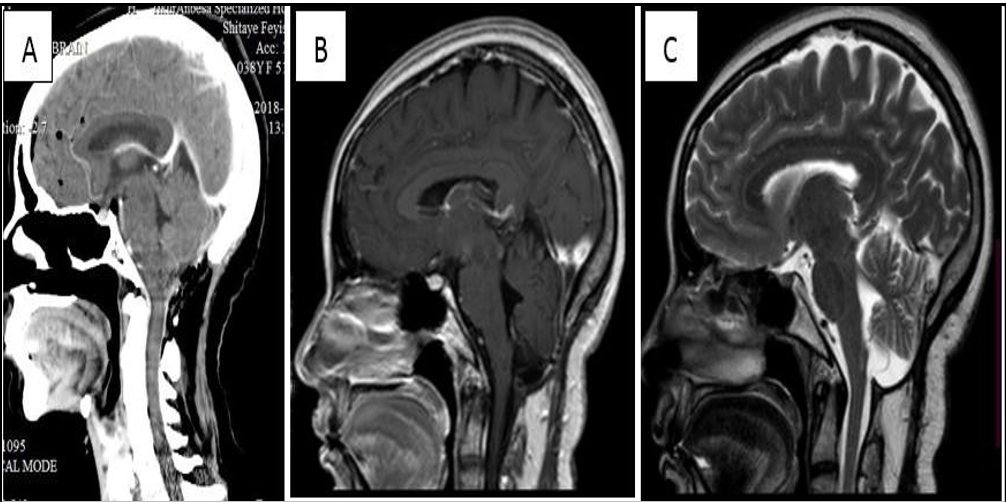
Figure 3: Immediate postoperative day head CT with contrast (A) and MRI at 6th month after surgery T1W sagittal image with gadolinium contrast (B) and T2W sagittal image (C) showed complete removal of the tumour with expected postoperative changes
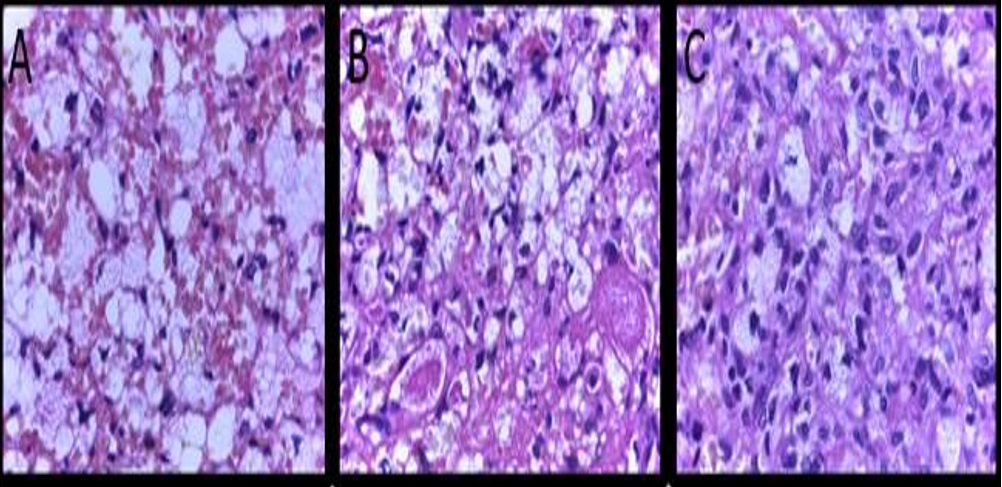
Figure 4: (A-C): Pathologic examination demonstrates proliferation of oval to spindle cells with hyper chromatic nuclei and some with foamy cytoplasm with accompanying thin-walled blood vessels consistent with hemangioblastoma
Discussions
Hemangioblastoma of the brainstem is a rare vascular benign neoplasm, with only a few reports of surgical treatment. The most frequent sites are the medulla oblongata and the fourth ventricle [4, 6]. Hence, hemangioblastoma of the brainstem can be classified based on these two sites in to three: I) Type A - those tumors attached to the floor of the fourth ventricle II) Type E - those tumors partially embedded in the dorsal medulla oblongata and III) Type I - intramedullary. The intramedullary hemangioblastoma is the least common type. Classifying based on this site may help to assess the surgical risks and predict the clinical outcome [4, 5]. The current case is intramedullary type.
About 70% of symptomatic brainstem hemangioblastomas are solid, in contrary to cerebellar hemangioblastomas in which 70% are cystic or with peritumoral cyst. Cystic brainstem hemangioblastomas or hemangioblastomas with peritumoral cyst, which develops due to increased vascular permeability of the hemangioblastoma resulting in extravasation of a plasma ultrafiltrate into the tumor interstitial spaces, are very rare with less than ten case reports [5, 7]. In addition to being intramedullary in location, the current case is also cystic in type with a small mural nodule to label it as one of the unique cases. Tumors in this anatomic region affects critical structures controlling respiration, swallowing and vomiting or may obstruct the CSF flow to cause hydrocephalus. The clinical presentation may vary depending on the location of the tumor. Features of raised ICP (headache, nausea and vomiting), unsteady gait, incoordination, and dysphagia are the most common symptoms at presentation. For obvious reason these symptoms were more frequent in the intramedullary type of brainstem hemangioblastomas than other types [4].
MRI with contrast is the investigation of choice for both the diagnosis and follow up of hemangioblastoma and is usually sufficient for preoperative evaluation. As these tumors are highly vascular, the solid part vividly and discretely enhances on T1-weighted MRI with gadolinium contrast. Peritumoral edema and cysts are best detected and monitored with fluid-attenuated inversion recovery (FLAIR) [3]. Cerebral angiography is recommended for large solid tumors, as it will allow a detailed study of the vascular anatomy and will help while planning of a surgical strategy in order to prevent catastrophic intraoperative bleeding [8, 9].
Safe gross total resection of the lesion is the ultimate goal of surgery. Since this tumors are highly vascular in a critical area, should be approached like arteriovenous malformation [10]. To facilitate easy en block tumor removal the feeding arteries should be coagulated first and the draining veins at last. Once the feeding arteries are coagulated and divided the tumor will start to shrink which aids to identify a cleavage plane between the tumor and the critical brainstem parenchyma [4]. To prevent massive intraoperative bleeding and to keep the surgical bed clean, en block removal of the tumor is recommended. Meticulous dissection of the tumor with no undue traction and gently rolling back and forth with bipolar coagulation to continuously reduce the size will allow en block removal of the tumor and minimizes postoperative complications. However, the removal of the cyst wall is not necessary as it is formed secondarily due to the increased vascular permeability of the tumor [10, 11].
Most importantly, to reduce the operative mortality and morbidity mainly from respiratory and circulatory complications, intensive postoperative care is mandatory [4, 10].
Conclusion
Intramedullary hemangioblastoma of the brainstem is a rare vascular neoplasm. En block removal of such tumors reduces the complications and improves the outcome of the patients. We report a case of intramedullary hemangioblastoma of the brainstem with a peritumoral cyst, which was managed surgically with good outcome. By increasing the availability of advanced neuroimaging and with improved microsurgical techniques, complete and safe resection of rare and difficult brain lesions like brainstem hemangioblastomas is possible in resource limited setups.
Authors’ contributions
All authors had involved in the process of edition and approved the final manuscript document
Abat Sahlu Baleh- Conceptualization, supervision, data curation, validation
Abdulaziz Abdellah Hussein- writing original draft, review editing, data curation
Murtii Teressa Obolu- Methodology, review editing, data curation, Software
Informed consent
Formal written informed consent is taken from patient for publications along with accompanying images, any identification part has been anonymised for the privacy and confidentiality of patients and it will be available up on request by journal chief editor.
Funding: No financing.
Conflict of interest: No conflict of interest in computation.
Acknowledgements
We would like to express our gratitude to the patients’ for providing informed consents for publication along with accompanying image and everyone else who helped with the intraoperative photo and the radiologic image collection.
References
- Conway JE CD, Clatterbuck RE, et al. (2001) Hemangioblastomas of the central nervous system in von Hippel-Lindau syndrome and sporadic disease. Neurosurgery. 48(1): 55-63.
- Temprano T, Fernández-de León R, Rial JC, Fernández JM, Mateos V (2008) Cystic bulbar hemangioblastoma. Rev Neurol. 47(3): 134-6.
- Zhou LF, Du G, Mao Y, Zhang R (2005) Diagnosis and surgical treatment of brainstem hemangioblastomas. Surg Neurol. 63(4): 307-15.
- Fukushima T, Sakamoto S, Iwaasa M, Hayashi S, Yamamoto M, et al. (1998) Intramedullary hemangioblastoma of the medulla oblongata--two case reports and review of the literature. Neurol Med Chir (Tokyo). 38(8): 489-98.
- Agrawal A, Kakani A, Vagh SJ, Hiwale KM, Kolte G (2010) Cystic hemagioblastoma brainstem. J Neurosci Rural Pract. 1(1): 20-2.
- Park DM, Zhuang Z, Chen L, Szerlip N, Maric I, et al. (2007) von Hippel-Lindau disease-associated hemangioblastomas are derived from embryologic multipotent cells. PLoS Med. 4(2): e60.
- Ammerman JM, Lonser RR, Dambrosia J, Butman JA, Oldfield EH (2006) Long-term natural history of hemangioblastomas in patients with von Hippel-Lindau disease J Neurosurg Pediatr. 105(2): 248-55.
- Wind JJ, Bakhtian KD, Sweet JA, Mehta GU, Thawani JP, et al. (2011) Long-term outcome after resection of brainstem hemangioblastomas in von Hippel-Lindau disease. J Neurosurg. 114(5): 1312-8.
- Liu X, Zhang Y, Hui X, You C, Yuan F, et al. (2015) Surgical management of medulla oblongata hemangioblastomas in one institution: an analysis of 62 cases. Int J Clin Exp Med. 8(4):5576- 90.
- Joseph J, Behari S, Gupta S, Bhaisora KS, Gandhi A, et al. (2018) Brain-stem hemangioblastomas: The seemingly innocuous lesion in a perilous location. Neurol India. 66(3): 779-96.
- Ma D, Wang Y, Du G, Zhou L (2015) Neurosurgical Management of Brainstem Hemangioblastomas: A Single-Institution Experience with 116 Patients. World Neurosurg. 4(84): 1030-8.