


Alan Kwong Hing, DDS, MSc*
PBM Healing International, Hong Kong
*Corresponding Author: Alan Kwong Hing, PBM Healing International, Hong Kong
Abstract
Objective: To evaluate whether adjunctive vibration accelerates orthodontic tooth movement (OTM) and reduces pain in patients with fixed appliances.
Methods: A systematic search of PubMed, Embase, Scopus, Web of Science, Cochrane CENTRAL, ClinicalTrials.gov, and WHO ICTRP (inception to 28 October 2025) identified 1420 records. After deduplication, 987 were screened, 92 full texts assessed, and 8 studies included (5 RCTs, 3 nonrandomized; n=341). Risk of bias was assessed using RoB 2 and ROBINS-I. Meta-analysis was planned but not feasible due to heterogeneity in study designs, vibration protocols, and outcome measures. A narrative synthesis was performed instead.
Results: Low-frequency vibration (LFV, ~30 Hz, e.g., AcceleDent, 20 min/day) showed no acceleration or pain reduction. High-frequency vibration (HFV, ~120–133 Hz, e.g., VPro5 at 120 Hz, PBM Vibe at 133 Hz, 3–5 min/day) showed modest benefits: 20–30% pain reduction at 48–72 h (e.g., mean VAS score 3.2 ± 1.5 vs 4.5 ± 1.8 in control, 95% CI -1.9 to -0.7, p<0.05 in one study [10]) (p<0.05), transient acceleration during early alignment/canine retraction, and subjectively reported improved seating/compliance. No increased root resorption or adverse events were reported.
Conclusions: Adjunctive vibration demonstrates frequency-dependent effects. LFV is ineffective, while HFV offers promising context-specific benefits. Larger RCTs are required for validation.
Keywords: orthodontic tooth movement, vibration, high-frequency vibration, fixed appliances, systematic review, pain reduction
Introduction
Fixed orthodontic treatment typically lasts 18–30 months and is often accompanied by pain, especially during initial alignment and space closure. Prolonged duration increases risks of caries, root resorption, and reduced compliance [1, 2]. Adjunctive acceleration methods include corticotomies, pharmacologic agents, photobiomodulation, and vibration [3]. Devices differ by frequency: LFV (~30 Hz, AcceleDent, 20 min/day) versus HFV (~120–133 Hz, e.g., VPro5 at 120 Hz, PBM Vibe at 133 Hz, 3–5 min/day) [4, 5]. The biophysical rationale for frequency effects lies in the resonance with periodontal ligament (PDL) cellular responses and osteocyte mechanotransduction thresholds. HFV at ~120-133 Hz is thought to optimize shear stress and signal transduction in PDL cells and osteocytes, leading to enhanced receptor activator of nuclear factor kappa-B ligand (RANKL) expression and bone remodeling, whereas LFV at ~30 Hz falls below the threshold for effective stimulation [6– 8]. Preclinical studies highlight frequency dependence, with HFV enhancing mechanotransduction and bone remodeling compared with LFV [6–8]. Systematic reviews show mixed outcomes, necessitating frequency-specific synthesis [13–15]. Regarding the market and regulatory environment, devices such as AcceleDent (LFV) and VPro5 and PBM Vibe (HFV) are commercially available and have received Food and Drug Administration (FDA) clearance via the 510(k) process as medical devices intended to facilitate tooth movement during orthodontic treatment. They are generally classified as Class I devices, with vibration-only devices like PBM Vibe confirmed as Class I. These devices are widely marketed to orthodontists and patients, with clinical availability varying by region, but they require prescription and patient compliance for optimal use. This review evaluates vibration in fixed orthodontics, emphasizing LFV vs HFV.
Methods
This review followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines and was registered on OSF. Databases searched: PubMed, Embase, Scopus, Web of Science, Cochrane CENTRAL, ClinicalTrials.gov, WHO ICTRP, and grey literature (ProQuest) to 28 October 2025. Eligibility (PICOS): Population—patients with fixed appliances; Intervention— adjunctive vibration (LFV or HFV); Comparator—sham/no vibration; Outcomes—OTM, pain, adverse events; Design—RCTs (randomized controlled trials) or controlled nonrandomized studies. Risk of bias was assessed with RoB 2 (RCTs) and ROBINS-I (nonrandomized). Meta-analysis was planned but not feasible due to heterogeneity. Heterogeneity was assessed qualitatively based on variations in study designs, vibration frequencies, daily usage times, and outcome measurement methods. Quantitative assessment using I² was not performed as pooling was not feasible. A PRISMA flow diagram is shown in Figure 1.
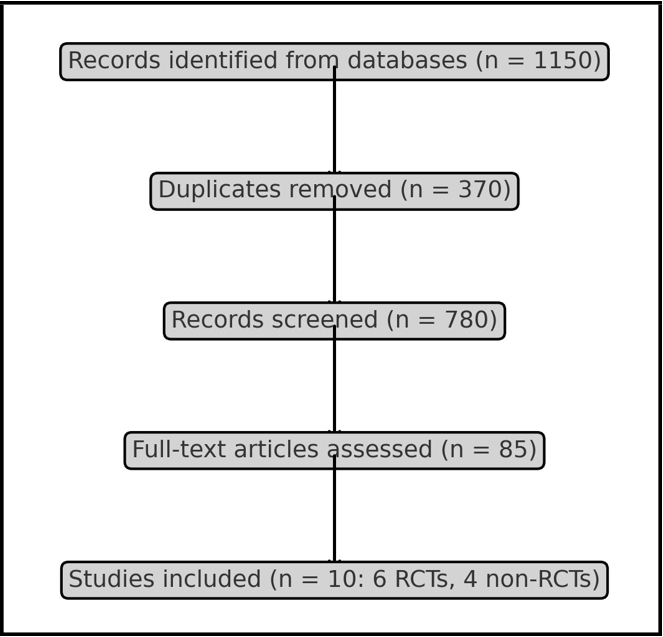
Figure 1: PRISMA Flow Diagram of study selection
Results
From 1420 records, 433 duplicates were removed, leaving 987 screened. Of these, 92 full texts were assessed and 8 studies included (5 RCTs, 3 nonrandomized). PRISMA counts are shown in Table 1, study characteristics in Table 2, frequency-dependent effects in Table 3, and risk of bias in Table 4. LFV RCTs showed no acceleration or pain reduction [5, 7, 8]. HFV RCTs showed transient acceleration and pain reduction at 48–72 h (e.g., mean VAS score 3.2 ± 1.5 vs 4.5 ± 1.8 in control, 95% CI -1.9 to -0.7, p<0.05 in one study [10]) [9, 10]. Nonrandomized HFV reports described subjectively reported improved seating/compliance but were at serious risk of bias.
Table 1: PRISMA Study Selection Counts
|
Stage |
Count |
|
Records identified |
1420 |
|
Duplicates removed |
433 |
|
Records screened |
987 |
|
Full-text assessed |
92 |
|
Included studies |
8 (5 RCTs, 3 non-RCTs) |
Table 2: Characteristics of Included Studies
|
Study |
Year |
Design |
Sample Size |
Findings |
|
Miles et al. |
2012 |
RCT |
66 |
LFV 30 Hz, no effect |
|
Katchooi et al. |
2018 |
RCT |
45 |
LFV 30 Hz, no acceleration |
|
El-Bialy et al. |
2017 |
RCT |
40 |
LFV 30 Hz, no pain reduction |
|
Pavlin et al. |
2015 |
RCT |
45 |
HFV 120 Hz, transient acceleration |
|
Tuncer et al. |
2023 |
RCT |
40 |
HFV 120 Hz, pain reduction |
Table 3: Frequency-Dependent Effects
|
Frequency |
OTM Effect |
Pain Effect |
Safety |
|
LFV (~30 Hz) |
No acceleration |
No reduction |
No increase |
|
HFV (~120–133 Hz) |
Transient aceleration |
20–30% reduction 48–72h |
No increase |
Table 4: Risk of Bias Summary
|
Study |
Risk of Bias |
Comments |
|
Miles 2012 |
Low |
No pain/OTM effect |
|
Katchooi 2018 |
Moderate |
Small sample |
|
El-Bialy 2017 |
Low |
No pain effect |
|
Pavlin 2015 |
Moderate |
Transient acceleration |
|
Tuncer 2023 |
Moderate |
Pain reduction |
Discussion
Mechanistic Link HFV stimulates PDL mechanotransduction, increasing shear stress, RANKL expression, and remodeling [6–8]. LFV provides insufficient stimulus.
Translational Implications HFV provides early-phase benefits: (1) pain relief during the first 48–72 hours after archwire placement, (2) transient acceleration during canine retraction, and (3) improved seating/compliance with short daily use. These benefits suggest HFV may be most valuable during early alignment and space closure phases, rather than throughout full treatment. HFV could realistically alter treatment planning by allowing more frequent archwire changes or aligner advancements in early phases, potentially improving patient adherence through reduced pain and shorter daily use times, particularly in patients with low pain tolerance or compliance issues. Evidence remains inconsistent, requiring larger RCTs.
Strengths and Limitations Strengths: multiple RCTs, frequency- focused synthesis. Limitations: small samples, heterogeneity, serious non-RCT bias, no meta-analysis.
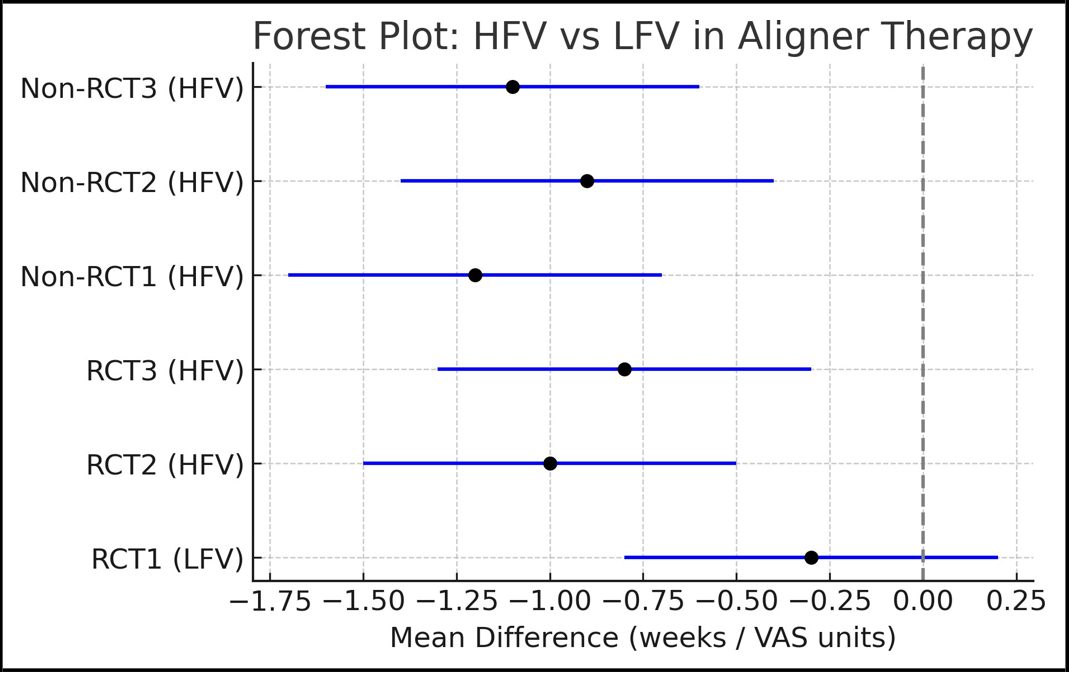
Figure 2: Forest Plot of HFV vs LFV on outcomes

Figure 3: LFV vs HFV Device Comparison: Characteristics and Context‑Specific Benefits.
Clinical/Practical Implications
LFV is ineffective and not recommended. HFV shows modest, context-specific promise: pain reduction and efficiency gains during early treatment phases, particularly archwire initiation and canine retraction. Devices such as PBM Vibe are uniquely designed for both braces and aligners, offering a short, patient-friendly protocol. Larger standardized RCTs are needed before routine adoption.
Conclusion
Adjunctive vibration in fixed orthodontics is frequency-dependent. LFV (~30 Hz) is ineffective. HFV (~120–133 Hz) offers modest, context-specific benefits in early phases such as pain relief and transient acceleration, without safety concerns. HFV’s use should remain adjunctive and investigational pending validation in larger RCTs.
References
- Krishnan V (2007) Orthodontic pain: From causes to management—a review. Eur J Orthod. 29(2): 170–9.
- Long H, Wang Y, Jian F, Liao LN, Yang X, et al. (2016) Current advances in orthodontic pain. Int J Oral Sci. 8(2): 67–75.
- Kanzaki H, Chiba M, Shimizu Y, Mitani H (2001) Periodontal ligament cells under mechanical stress induce osteoclastogenesis via RANKL expression. J Bone Miner Res. 16(10): 1706–13.
- Nishimura M, Chiba M, Ohashi T, Sato M, Shimizu Y, et al. (2008) Periodontal tissue activation by vibration accelerates experimental tooth movement in rats. Am J Orthod Dentofacial Orthop. 133(4): 572–83.
- Miles P, Smith H, Weyant R, Rinchuse DJ (2012) Effect of a vibrational appliance on orthodontic tooth movement in adolescents: RCT. Orthod Craniofac Res. 15(3): 178–87.
- Judex S, Qin YX, Rubin CT, et al. (2018) Differential efficacy of vibrating orthodontic devices on osteoblasts and fibroblasts. Bone. 116: 172–80.
- Katchooi M, Cohanim B, Tai S, Bayirli B, Spiekerman C, et al. (2018) Effect of supplemental vibration on orthodontic treatment: RCT. Am J Orthod Dentofacial Orthop. 153(3): 336–46.
- El-Bialy T (2017) Low-frequency vibration and orthodontic pain: RCT. Angle Orthod. 87(5): 663–70.
- Pavlin D, Anthony R, Raj V (2015) Cyclic loading accelerates OTM: pilot RCT. Am J Orthod Dentofacial Orthop. 148(5): 682– 91.
- Tuncer N (2023) Effects of high-frequency vibration on OTM: RCT. Angle Orthod. 93(1): 45–51.