


Abdi Tesemma1*, Galaye Fekadu2, Kebebe Bekele1, Miheret Adane3, Girma Beressa4, Abdulhafiz Mohammed5
1Department of Surgery, Madda Walabu University, Goba, Ethiopia
2Department of Ophthalmology, Madda Walabu University, Goba, Ethiopia
3School of Health Science, Madda Walabu University, Goba, Ethiopia
4Public Health, Madda Walabu University, Goba, Ethiopia
5University of North Carolina Gillings School of Public Health, Carolina, USA
*Corresponding Author: Abdi Tesemma, Department of Surgery, Madda Walabu University, Goba, Ethiopia.
Abstract
Background: Facial palsy is the paralysis of muscles in the face. Paralysis is usually unilateral. It has various causes, such as Bell’s palsy, trauma, infection, and autoimmune and congenital effects. Bell’s palsy is the most common cause of facial palsy. Trauma is also the major cause of facial palsy. On rare occasions, minor trauma to the face can result in facial palsy, and professional diagnosis and empirical treatment with steroids and eye care are options for managing this condition in resource-limited areas.
Patient presentation: A 65-year-old Ethiopian male presented to Goba Referral Hospital with the inability to close his left eye and drooping his mouth following minor facial trauma caused by a piece of wood on his left side of the face while making a burning wood two days prior to his presentation at the hospital. With a professional diagnosis of facial palsy following minor facial trauma, the patient was treated with steroids and eye care and achieved good recovery.
Conclusion: We conclude that the ideal management of facial palsy secondary to minor face trauma in resource-limited patients is professional diagnosis and conservative treatment with steroids and eye care with close follow-up.
Keywords: Facial palsy, Bell’s palsy, Minor trauma, Eye care, Ethiopia
Introduction
Facial palsy is a temporary acute weakness of the facial muscle on one side in most cases. Bell’s palsy is the most common cause of acute peripheral, unilateral, lower motor lesions of cranial nerves. The lesion can be partial (paresis) or complete (paralyse) [1, 2]. Bell’s palsy is the most common cranial nerve neuropathy and the most common cause of facial weakness worldwide; it occurs in 60-75% of all cases of facial palsy [2]. The annual incidence of Bell’s palsy is 7- 40 per 100,000 people [2]. Bell’s palsy is a diagnosis of exclusion in cases of unknown cause [1]. Facial palsy has no sex or ethnic prediction and can occur at all ages. The recurrence rate of facial palsy is estimated to be between 4% and 14%. Regardless of the cause, facial palsy gradually resolves in some function over time in approximately 85% and completely resolves in 70% of cases [1, 3]. Facial nerve weakness can occur following trauma, viral infection, such as herpes simplex virus (most likely of unknown cause), tumors, autoimmune disease and congenital disease [1, 2, 3, 4, 5, 6, 7]. On rare occasions, minor trauma to the face can result in facial palsy, and some cases have been reported [4].
The presentation of facial palsy can be sudden, occurring within 48 h, and involves both the upper and lower faces [1, 2].Patients with this type of lesion present with ipsilateral difficulty in closing the eye, dryness, drooping of the mouth, an inability to wrinkle the brow and loss of the nasolabial fold, asymmetrical smile and facial muscle tone [1, 8].
Facial nerve palsy following trauma to the face can manifest immediately within 48 hr of insult or after a delay of days to weeks [2]. The signs and symptoms depend on the severity of the injury and the clinical classification of facial nerve function [1]. The same clinical pattern of facial palsy occurs with minor trauma in rare scenarios [4]. The diagnosis of facial palsy is based on the patient’s clinical history and physical examination [4, 5]. Diagnostic tests and imaging modalities are performed to confirm the diagnosis and rule out other disease conditions [1, 2, 4,7 , 9].
The management of facial palsy in patients with minor facial trauma is conservative, with most patients receiving steroid and eye care even in the absence of radio imaging [1, 3, 4, 8]. In this article, we present a rare case report of facial palsy following minor facial trauma. The patient was managed with steroids and eye care with tear lubricants and nocturnal eyelid taping. The symptoms started to improve within one week of treatment and resolved gradually over four to six weeks.
Case Presentation
A 65-year-old Ethiopian male farmer presented to Goba Referral Hospital with complaints of the inability to close his left eye and drooping of the mouth following minor facial trauma caused by a piece of wood on his left side of the face while making a burning wood two days prior to his presentation. He also complained of a burning sensation, increased tearing, blurring of vision from the left eye, difficulty chewing food and leakage of food and drinks from the left side of the mouth. The patient was relatively healthy and had no similar symptoms prior to the incident of minor trauma. There was no history of headache, fever, ear or eye discharge, mastoid or per auricular pain, or difficulty swallowing or aspiration. He had no trauma to the head, any limb weakness or history of weight loss.
The patient denied any viral infection, such as mumps, herpes zoster or HIV. He had no underlying medical illness, namely, diabetes mellitus or cardiac or hypertension, in the past and presented and did not take any medicine.
Clinical examination revealed a PR of 75 bpm, a RR of 15 pm, a BP of 120/70 mmHg, and a T 36.2 C weight of 72 kg. On ear examination, all Weber, Rene, and otoscopy tests yielded positive results.
Facial deviation to the right and the absence of a left brow crease (Figure 1), ptosis and incomplete closure of the left eyelid resulted in a 2 mm gap and mild lagophthalmos (Figure 2). Slit lamp microscopy examination of the left eye revealed temporal interpalperal bulbar conjunctiva injection and lustre and uneven inferior corneal surfaces. Bell’s phenomenon was positive.
Taste and salivation affected the left side of the tongue, and air leaked upon blowing the check from the left side and could not blow the check (Figure 3). House and Brackman grading results in severe dysfunction.
The other systemic physical examination was unremarkable.
The complete blood count and biochemical test results were within the normal range. Viral markers, including HIV, are nonreactive.
A CT scan of the head was planned for further evaluation. In addition, the patient opts to receive empirical treatment from the professional diagnosis because of radio imaging unavailability in our hospital and the patient’s inability to afford referral. With the clinical or professional diagnosis of left facial palsy following minor facial trauma, oral prednisone 60 mg/day for one week, 50 mg/day for one week, 40 mg/day for one week, 30 mg/day for one week, 20 mg/day for one week, 10 mg/kg for one week, and 5 mg/day for one week was given, and the treatment was stopped. Eye treatment included nocturnal eyelid taping for one week, treatment with 1% tetracycline eye ointment at bed for one week, and natural tear eye drops (carboxymethylcellulose) qid/day for 4 weeks. There was improvement in the left brow crease and eyelid color within four weeks (Figure 4a and b). The palsy completely resolved after four to six weeks of treatment. The patient was followed for 2nd months and then every three months for the last one and a half years, with good recovery and no recurrence of palsy (Figure 5).

Figure 1: Absent left brow crease and deviation of the face to the right.
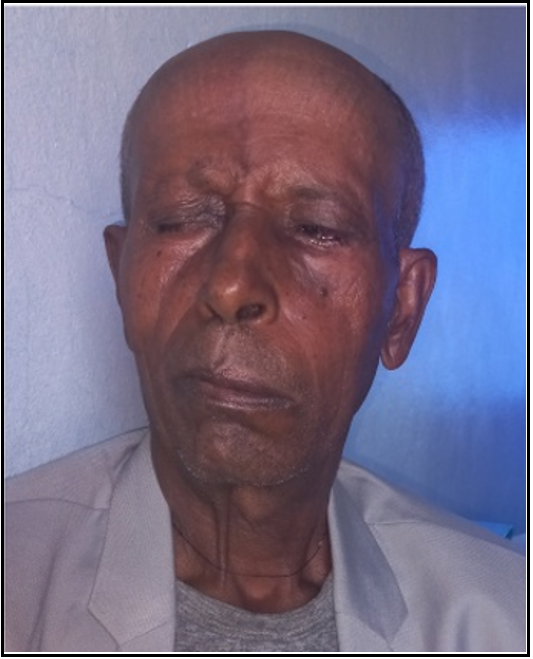
Figure 2: The ptosis and incomplete view of the left eyelid measure a 2 mm gap, with mild lagophthalmos.

Figure 3: shows that air leaks upon blowing the check from the left side and cannot blow the check.

Figure 4a: Retaining of the left brow crease.
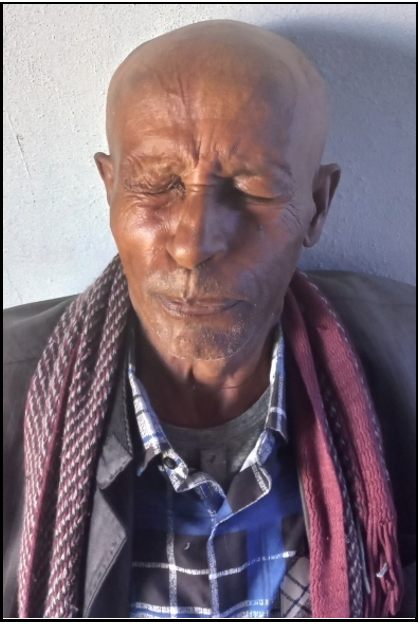
Figure 4b: Closer view of the left eyelid with mild ptosis.

Figure 5: Closure of the eyelid, normal brow crease and absence of facial deviation.
Discussion
Trauma to the face can result in physiological dysfunction and cosmetic problems as a result of a lack of innervations and an asymmetric tone. Here, we discuss a rare case of facial palsy caused by minor facial trauma caused by a piece of wood on his left side of the face while he was making firewood. The patient was diagnosed clinically and managed via an empirical approach [3, 4].
Facial palsy results from damage to cranial nerve VII, which innervates muscles of the face. There are two types of facial palsy based on the location of damage. Central and peripheral facial palsy are caused by damage above and below the facial nucleus, respectively [10]. The causes of peripheral facial palsy can be categorized into upper and lower neuron lesions [7]. The lower neuron lesions are idiopathic or Bell’s palsy (the most common cause of facial palsy), tumors, infections, trauma, congenital and other rare causes [5, 11]. In our case, the damage to the peripheral lower motor lesion of the facial nerve was managed conservatively after clinical diagnosis [1, 2, 3, 4, 6].
Trauma to the head and face, especially fractures of the temporal, mastoid and zygomatic bones, results in facial palsy where the facial nerve passes through [2,6,12]. Imaging modalities of the head can reveal the location of damage and underlying causes with other investigations and clinical presentations [3, 5, 6]. We settled the diagnosis professionally as a result of the unavailability of imaging modalities in our setup and the patient’s inability to afford referral.
The patient was put on oral prednisone 60 mg per day by tapering weekly for six weeks, and eye care with a carboxymethylcellulose drop was given daily for two weeks, and nocturnal eye tapering for one week. Incomplete facial nerve injury can respond to conservative management. Surgery might be mandatory for patients with underlying causes of tumors. Antiviral and antibiotic prescriptions are routinely given for viral or bacterial causes [1, 2, 5, 6]. In our case, the patient responded to oral steroids and eye care with resolution of palsy over four to six weeks of treatment. In resource-limited areas, we can approach patients clinically and manage them empirically with strict follow-up.
The presentation of facial palsy in trauma to the head and face can be early within 48 hrs or delayed for days to weeks. An appropriate history in a systematic manner and physical examination, particularly in resource-limited regions of the world, can guide professional diagnosis and management accordingly [4, 13].
In patients with Bell’s palsy, acyclovir in addition to steroids is needed even though the cause is unknown or idiopathic because it is usually related to viral infection, such as herpes simplex virus infection [1, 13]. This palsy usually resolves over several weeks. There are risk factors for Bell’s palsy, namely, third trimester pregnancy, diabetes mellitus, upper respiratory tract infections, and hypertension, which also require a multidisciplinary approach and clinical judgment to manage per se [1, 2, 3, 6].
To summarize our discussion of facial palsy following minor trauma, a good clinical approach and judgment for management with strict or close follow-up even in the absence of radiological imaging are needed. Standard laboratory investigations and imaging, in addition to physical diagnosis, constitute the best setup for facial palsy diagnosis, treatment and follow-up [9]. However, in resource-limited areas, such as our set-up, the clinical approach and empirical treatment constitute the mainstays for the management of facial palsy with close follow-up [3]. Close follow-up is mandatory; hence, palsy may improve or worsen.
Conclusion
Any trauma, including minor facial trauma is likely to result in facial palsy. A high index of clinical suspension is mandatory for clinical diagnosis and managing patients with oral steroids and eye care with lubricants and nocturnal eyelid taping is highly recommended. Close follow-up for the resolution of symptoms in conservative management in resource-limited areas.
Acknowledgment
The authors are grateful to the Surgery and Ophthalmology Department staff for their efforts in conservative management and follow-up of the patient.
Authors’ Contributions
The AT was involved in various aspects of the case, including patient diagnosis, management, idea, formal analysis, investigation, methodology, supervision, validation, writing the original document, conducting the review, and editing. GF was involved in ocular examination and patient management, and in review and editing. KB was involved in supporting the idea and assisting in the writing of the original document. MA, GB and AH were involved in the validation, substantive review, and extensive editing. All the authors reviewed and approved the manuscript.
Declarations: No
Funding Source: None
Conflict Of Interest: The authors declare that they have no competing interests.
Ethics Approval
As our institution does not need ethical approval for case reports, no ethical approval is needed.
Consent To Participate
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Availability Of Data And Material
The data that supports the findings of this study will be made available to anyone by contacting the corresponding author.
References
- Baugh RF, Basura GJ, Ishii LE, Schwartz SR, Drumheller CM, et al. (2013) Clinical practice guideline: Bell's palsy. Otolaryngol Head Neck Surg. 149(3 Suppl): S1-27.
- Singh A, Deshmukh P (2022) Bell's Palsy: A Review. Cureus. 14(10): e30186.
- Garro A, Nigrovic LE (2018) Managing Peripheral Facial Palsy. Ann Emerg. 71(5): 618-624.
- Ghimire R (2021) An unusual case of facial nerve palsy due to minor face trauma: A rare case report. SAGE Open Med Case Rep. 9: 1-5.
- Jowett N (2018) A General Approach to Facial Palsy. Otolaryngol Clin North Am. 51(6): 1019-1031.
- Greiner RC, Kohlberg GD, Lu GN (2024) Management of facial nerve trauma. Curr Opin Otolaryngol Head Neck Surg. 32(4): 234-238.
- Kim SJ, Lee HY (2020) Acute Peripheral Facial Palsy: Recent Guidelines and a Systematic Review of the Literature. J Korean Med Sci. 35(30): e245.
- Pereira MV, Glória AL (2010) Lagophthalmos. Semin Ophthalmol. 25(3): 72-78.
- Kim TH, Yeo SG, Byun JY (2021) Role of Biomarkers as Prognostic Factors in Acute Peripheral Facial Palsy. Int J Mol Sci. 23(1): 307.
- Seneviratne SO, Patel BC (2025) Facial Nerve Anatomy and Clinical Applications.Treasure Island (FL): StatPearls Publishing.
- Zhu YH, Han WJ (2019) [Congenital facial palsy]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 54(10): 787-791.
- Lam AQ, Chung TTP, Viet TL, Quang DH, Van TD, et al. (2022) The Anatomic Landmark Approach to Extratemporal Facial Nerve Repair in Facial Trauma. Cureus. 14(3): e22787.
- Robinson MW, Baiungo J (2018) Facial Rehabilitation: Evaluation and Treatment Strategies for the Patient with Facial Palsy. Otolaryngol Clin North Am. 51(6): 1151-1167.